To Study The Effect of Type 2 Diabetes Mellitus and Glycaemic Index on Hearing
Gulati A1*, Kakkar V1, Aggarwal S2, Panchal V1, Pareek M1, Aman1
1 Department Of Otorhinolaryngology, PGIMS, University of Health Sciences, Rohtak, India.
2 Department Of Medicine, PGIMS, University of Health Sciences, Rohtak, India.
*Corresponding Author
Dr. Ankit Gulati,
Department Of Otorhinolaryngology,
PGIMS, University of Health Sciences, Rohtak, India.
E-mail: gulati.ankit07@gmail.com
Received: September 09, 2017; Accepted: September 25, 2017; Published: September 27, 2017
Citation: Gulati A, Kakkar V, Aggarwal S, Panchal V, Pareek M, Aman. To Study The Effect of Type 2 Diabetes Mellitus and Glycaemic Index on Hearing. J Translational Clin Case Rep Fam Physician. 2017;3(1):19-22.
Copyright: Gulati A© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: This study has been undertaken to study the effect of Type 2 diabetes mellitus and Glycaemic index on hearing.
Methods: The present study was conducted on 200 persons of age group 20-45 years. All subjects included in the study were divided into two groups. Group I: 100 patients suffering from T2DM (fasting blood sugar ≥ 126mg/dl and postprandial ≥ 200mg/dl) of either sex, in the age group of 20 to 45 years. Group II: 100 healthy volunteers in the age group of 20 to 45 years, of either sex were included in control group. Hearing assessment was done by using Pure Tone Audiometry.
Results: In diabetics patients, the mean threshold in the pure tone audiometry was higher at all frequencies as compared to healthy controls and there was no correlation between the glycaemic index and hearing loss.
Conclusions: The prevalence of sensorineural hearing loss in type II diabetics observed was 64%. In the majority of the patients the hearing loss was bilateral affecting mid and higher frequencies from 2 KHz to 8 KHz. Hence to conclude we can say that the high prevalence of hearing loss in T2DM supports the importance of audiometric evaluation in such patients.
2.Introduction
3.Methods
3.1 Inclusion Criteria
3.2 Exclusion Criteria
4.Audiological Assessment
5.Statistical Analysis
6.Results
6.1 Hearing Loss
6.2 SNHL And Glycaemic Control (Group I)
7.Discussion
7.1 Hearing loss in T2DM
7.2 Effect of T2DM on Pure Tone Audiometry
7.3 Glycaemic Control and Hearing Loss
8.Summary And Conclusion
9.References
Keywords
Type 2 Diabetes Mellitus; Pure Tone Audiometry; Sensorineural Hearing Loss.
Introduction
Diabetes mellitus (DM) is a syndrome characterized by disordered metabolism and inappropriate hyperglycemia due to either a deficiency of insulin secretion or to a combination of insulin resistance and inadequate insulin secretion to compensate. DM is classified into Type 1 DM (T1DM) and Type 2 DM (T2DM) [1]. T2DM is more prevalent form and results from insulin resistance with a defect in compensatory insulin secretion [2]. Chronic complications associated with DM are microvascular complications i.e., nephropathy, neuropathy, retinopathy and macrovascular complications such as coronary artery disease, peripheral vascular disease [3].
In DM, the hearing impairment is predominantly bilateral senorineural hearing loss (SNHL) mainly affecting high frequency tones with a gradual onset and progression [4]. Suggested pathogenesis for this DM-associated SNHL includes cochlear microangiopathy, hyperglycemia of the cerebrospinal fluid or perilymph, auditory neuropathy, and diabetic encephalopathy [5]. Changes in central auditory and cognitive processing have also been documented in subjects with diabetes [6].
With this background present study was undertaken to study the effect of T2DM on hearing and to assess whether hearing impairment is associated with glycaemic control of T2DM.
Methods
The present study was conducted in the Department of Otorhinolaryngology in collaboration with Department of Medicine Pt. B.D. Sharma PGIMS, Rohtak in 200 persons of age group 20-45 years. All subjects included in the study were divided into two groups.
Group I: 100 patients suffering from T2DM (fasting blood sugar ≥ 126 mg/dl and postprandial ≥ 200 mg/dl) of either sex, in the age group of 20 to 45 years.
Group II: 100 healthy volunteers in the age group of 20 to 45 years, of either sex were included in control group.
Patient in the age group of 20 to 45 years having T2DM for more than 1 year.
• Patient <20 years or > 45 years.
• Subjects having conductive hearing loss, otitis externa and tympanic membrane perforation.
History of any ear discharge, ototoxic drug intake, impairment of hearing and family history of deafness, meningitis, encephalitis, head injury and patients having congenital anomalies of auricle or external auditory meatus.
All patients underwent detailed evaluation based on history, general physical examination as well complete ear nose throat examination. Pure tone audiometry (PTA) was done for assessing the effect of T2DM on hearing. HbA1c was used to assess the glycaemic control & values available within past three months were recorded. An informed consent was taken to participate in the study.
Audiological Assessment
The pure-tone audiometry was conducted using ALPS AD 2000 + audiometer to measure the air conduction thresholds at the octave frequencies between 250 Hz-8000 Hz with a 10 dB up and 5 dB down threshold seeking procedure. Bone conduction thresholds were measured at 250 Hz-8000 Hz using the same procedure.
Statistical Analysis
The data collected in the study was compiled and analyzed by using unpaired and paired students ‘t’ test and chi square test.
p value > 0.05 was considered as not significant (NS).
p value < 0.05 was considered as significant (S).
p value < 0.01 was considered as highly significant (HS).
p value < 0.001 was considered as very highly significant (VHS).
Results
The age group of cases and controls in our study was between 20 to 45 years with most of them between 31 to 35 years. The difference in sex distribution between two groups was insignificant ( p > 0.05).
The difference in hearing threshold at frequency ranging from 250 Hz to 8k of both right and left ears for air conduction between group I and group II was statistically very highly significant (p<0.001). There was mild hearing loss at 2k, 4k and 8k frequencies.
The difference in hearing threshold at frequency ranging from 250 Hz to 8k of both right and left ears for bone conduction between group I and group II was statistically very highly significant (p<0.001). (Table 1)
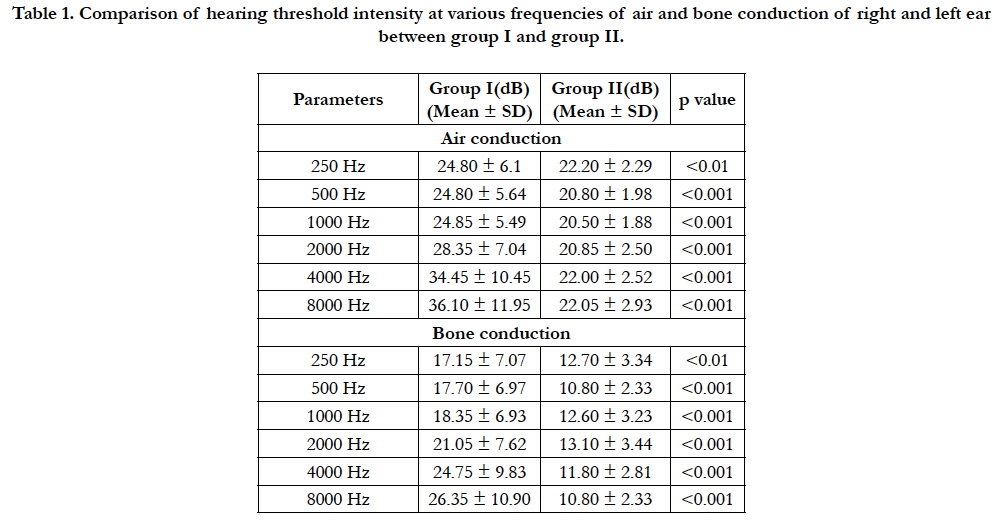

Table 1. Comparison of hearing threshold intensity at various frequencies of air and bone conduction of right and left ear between group I and group II.
Hearing Loss
In Group I, sixty four (64%) subjects had bilateral sensorineural hearing loss with an average AC threshold of 31.78 dB in right ear and 31.95 dB in left ear, average BC threshold of 24.75 dB in right ear and 24.76 dB in left ear with average A-B gap 6.5 dB in right ear and 6.4 dB in left ear. Four patients had unilateral mixed hearing loss (4%) while thirty two (32%) had no hearing loss while in Group II, no hearing loss was observed.(Figure 1)
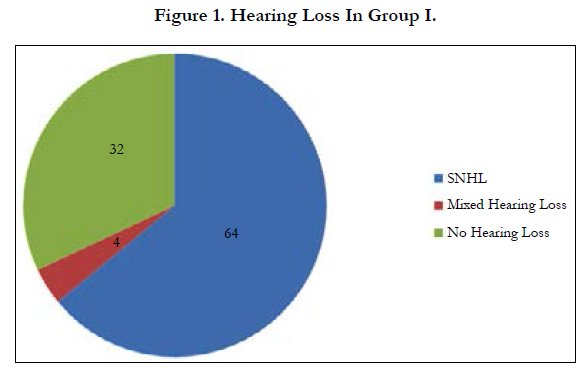
Figure 1. Hearing Loss In Group I.
SNHL And Glycaemic Control (Group I)
Sixteen patients (66.7%) out of twenty four having HbA1c <7 gm% , thirty two patients (80%) out of forty HbA1c 7-8 gm% while sixteen patients (44.4 %) out of thirty six having HbA1c > 8 gm% had bilateral sensorineural hearing loss.
Mean air conduction thresholds at various frequencies does not increases with increase in HbA1c showing no correlation of hearing threshold with the glycaemic control. (Table 2 and Figure 2).
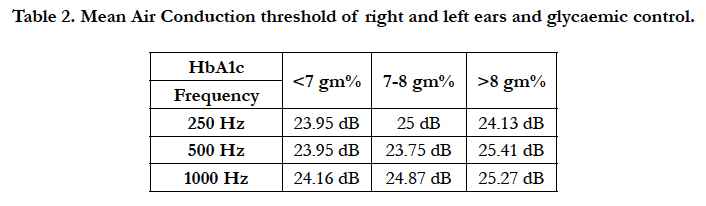
Table 2. Mean Air Conduction threshold of right and left ears and glycaemic control.
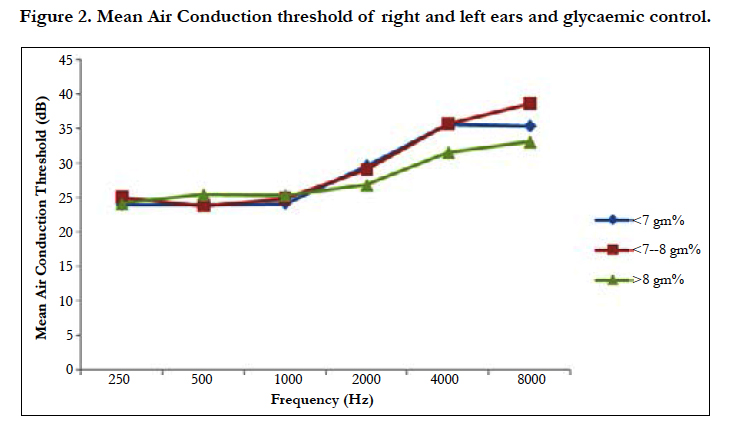
Figure 2. Mean Air Conduction threshold of right and left ears and glycaemic control.
Discussion
The relationship between diabetes mellitus and hearing loss is complex and under debate since many years supported by the bulk of conflicting literature. The crux about the effect of diabetes on hearing loss lies centered around the cochlea and the neural pathways, which have been studied through the years in relation to age, sex, duration and glycaemic levels.
Hearing loss in T2DM
In our study involving 100 subjects of type 2 diabetes, the prevalence of hearing loss was found to be 68% out of which 64% had bilateral sensorineural hearing loss while 4 % had unilateral mixed hearing loss. The results approximates to those that of Friedman et al., [7] (55%) and Aggarwal et al., [8] (64.86%) while Pani et al., [9] reported a higher incidence of hearing loss (80%). There is wide variation of results regarding the prevalence of SNHL in diabetics due to different inclusion and exclusion criteria, methodology and diagnostic approaches.
Effect of T2DM on Pure Tone Audiometry
As shown in Table 1, the cases showed gradual increase in hearing threshold starting at 250 Hz and becoming pronounced as the frequency increased whereas all the controls had normal hearing threshold. Frisina et al also observed that with increasing frequency, threshold sound intensity increases in diabetic subjects [10]. The results of our study also supports Austin et al., who observed that individuals with T2DM have significantly worse hearing (higher mean pure tone thresholds) than those with no DM across all test frequencies [5].
Mild hearing loss was observed for frequencies 2k, 4k and 8k. The results approximates with that of Pani et al., [9] and Tay et al., [11] who also observed hearing loss in mid and high frequencies. In contrast Kurien et al., [12] and Cullen et al., [13] observed hearing loss in higher frequencies. Fangchao et al., observed hearing loss only at 500 Hz [14]. Salvenelli et al., did not find hearing loss in the diabetic subjects [15]. The possible pathophysiological basis for this reduction in auditory acuity may be; microangiopathy of the inner ear, neuropathy of the cochlear nerve, or a combination of both. Several studies have attempted to locate the site of any possible pathological processes causing hearing loss in diabetics. Thickened capillaries in the stria vascularis, basilar membrane, and endolymphatic sac were also observed. They also proposed that these changes were responsible for diabetic SNHL [16]. Similar microangiopathic mechanisms were proposed by Kakarlapudi et al., [17] and Zelenka et al., [18] who found sensorineural hearing loss in all the frequencies tested in their diabetic subjects.
Glycaemic Control and Hearing Loss
The control of blood sugar levels and hearing loss has been the most controversial and to ponder over this the glycated haemoglobin (HbA1C) has been taken into account. HbA1C was taken into consideration since it directly gives an idea about the blood sugar control of the patient in the previous 3 months. There was no correlation observed between glycaemic control and hearing loss in our study. Dalton et al [19], Salvanelli et al., [15] and Rajendran et al., [20] also observed that glycaemic control has no effect on the incidence of hearing loss in diabetic patients. On the contrary Pani et al., [9] and Panchu et al., [21] observed a positive correlation between the glycaemic control and hearing loss. As short term sugar control cannot predict the effect on the pathology involved and absence of diagnostic means to directly measure the metabolic control on long term, can be a possible reason for the above observation in our study.
Summary And Conclusion
Diabetes mellitus is an endocrine disorder affecting multiple organ systems especially neural component. Various audiological investigations have revealed that there is a strong association of diabetes with sensorineural part. The prevalence of sensorineural hearing loss in type II diabetics observed was 64%. In the majority of the patients the hearing loss was bilateral affecting mid and higher frequencies from 2 KHz to 8 KHz. Hence to conclude we can say that the high prevalence of hearing loss in T2DM supports the importance of audiometric evaluation in such patients.
References
- Rother KI. Diabetes treatment-bridging the divide. N Engl J Med. 2007 Apr 12;356(15):1499-501. PubMed PMID: 17429082.
- Papadakis AM, Mcphee JS, Rabow WM. Current Medical Diagnosis And Treatment. 50th edn. New York: McGraw-Hill Lange; 2010.
- Sarkar RN, Banerjee S, Basu AK, Bandyopadhyay D. Rheumatological manifestations of diabetes mellitus. J Indian Rheumatol Assoc. 2003;11:25-9.
- Lisowska G, Namysłowski G, Morawski K, Strojek K. Early identification of hearing impairment in patients with type I diabetes mellitus. Otol Neurotol. 2001 May;22(3):316–20. PubMed PMID: 11347633.
- Austin DF, Konrad-Martin D, Griest S, McMillan GP, McDermott D, Fausti S. Diabetes-related changes in hearing. Laryngoscope. 2009 Sep;119(9):1788-96. PubMed PMID: 11318468.
- Lisowska G, Namyslowski G, Morawski K, Strojek K. Cochlear dysfunction and diabetic microangiopathy. Scand Audiol Suppl. 2001;30(52):199–203. PubMed PMID: 11318468.
- Friedman SA, Schulman RH, Weiss S. Hearing and diabetic neuropathy. Arch Intern Med. 1975 Apr;135(4):573-6. PubMed PMID: 1138672.
- Aggarwal NK, Jha A, Singh SK. Otorhinolaryngological studies in diabetics. Indian J Otolaryngol Head Neck Surg. 1998 Apr;50(2):116-20. PubMed Central PMCID: 3450990.
- Pani Veena MK, Swathi VM, Jasmine A. Effect of early onset type 2 diabetes mellitus on hearing. Evol Med Dental Sci. 2013 Nov 18;2(46):8880-5.
- Frisina ST, Mapes F, Kim S, Frisina DR, Frisina RD. Characterization of hearing loss in aged type II diabetics. Hear Res. 2006 Jan;211(1-2):103-13. PubMed PMID: 16309862.
- Tay HL, Ray N, Ohri R. Diabetes mellitus and hearing loss. Clin Otolaryngol. 1995 Apr;20(2):130-4. PubMed PMID: 7634518.
- Kurien M, Thomas K, Bhanu TS. Hearing threshold in patients with diabetes mellitus. J Laryngol Otol. 1989 Feb;103(2):164-8. PubMed PMID: 2926261.
- Cullen R, Cinnamond NJ. Hearing loss in diabetes. J Laryngol Otol. 1993 Mar;107(3):179-182. PubMed PMID: 8509689.
- Fangcha MA Gomez-Marin O, Lee DJ, Balkany T. Diabetes and Hearing Impairment in Mexican American Adults: a population-based study. J Laryngol Otol. 1998 Sep;112(9):835-9. PubMed PMID: 9876372.
- Salvenelli F, Miele A, Casale M, Greco F, D’Ascanio L, Firrisi, et al. Hearing thresholds in patients with diabetes. Internet J Otorhinolaryngol. 2004;3(1).
- Wackym PA, Linthicum FH Jr. Diabetes mellitus and hearing loss: clinical and histopathological relationships. Am J Otol. 1986 May;7(3):176-82. PubMed PMID: 3717308.
- Kakarlapudi V, Sawyer R, Staecker H. The effect of diabetes on sensorineural hearing loss. Otol Neurotol. 2003 May;24(3):382-6. PubMed PMID: 12806288.
- Zelenka J, Kozac P. Disorders in blood supply of the inner ear as early symptom of diabetic angiopathy. J Laryngol Otol. 1965 Apr;79:314-9. PubMed PMID:14279154.
- Dalton SD, Cruickshanks KJ, Klein R, Klein BE, Wiley TL. Association of NIDDM and hearing loss. Diabetes Care. 1998 Sep;21(9):1540–4. PubMed PMID: 9727906.
- Sambandam R, Anandhalakshmi, Mythili, Rao V. Evaluation of the incidence of sensorineural hearing loss in patients with type 2 diabetes mellitus. Int J Biol Med Res. 2011;2(4):982-7.
- Panchu P. Auditory acuity in type 2 diabetes mellitus. Int J Diabetes Dev Ctries. 2008 Dec;28(4):114-20. PubMed Central PMID: PMC2822154.





