Predictive Value of COPD: Impulse Oscillometry In Detective of Airway Resistance and Reactance In Chinese Elderly
Chen B, Zou C*, Wang X, Wu J*
Department of Geriatrics, The First Affiliated Hospital of Nanjing Medical University, Guangzhou Road, Nanjing, China.
*Corresponding Author
Jianqing Wu,
Department of Geriatrics, The First Affiliated Hospital of Nanjing Medical University,
300 Guangzhou Road, Nanjing 210029, China.
Tel/Fax: +86 25 68135113
E-mail: jwuny@njmu.ed.cn
Chunying Zou,
Department of Geriatrics, The First Affiliated Hospital of Nanjing Medical University,
300 Guangzhou Road, Nanjing 210029, China.
E-mail: 13851791763@163.com
Received: September 17, 2016; Accepted: October 04, 2016; Published: October 13, 2016
Citation: Chen B, Zou C, Wang X, Wu J (2016) Predictive Value of COPD: Impulse Oscillometry In Detective of Airway Resistance and Reactance In Chinese Elderly. J Translational Biomarkers Diagn. 2(1), 9-14.
Copyright: Wu J, Zou C© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Impulse oscillometry (IOS) can be complementary to spirometry, especially in patients at advanced age and with physical or mental disorders who cannot successfully perform spirometry. The aim of this study was to compare IOS and spirometry in the assessment of airway obstruction in COPD. The study was conducted in 141 stable COPD patients and 126 healthy subjects with normal spirometry. The oscillometric evaluation included total resistance (R5), proximal resistance (R20), distal capacitive reactance (X5), peripheral resistance (R5-R20) and resonance frequency (Fres) , which were compared with the predicted forced expiratory volume in 1 second (FEV1%pred). Correlations between the severity of airway obstruction (FEV1%pred) and respiratory resistances and reactance were calculated. Receiver operating characteristics (ROC) curve analysis was also performed to evaluate the diagnostic ability of each of the IOS measurements for COPD. The findings show a significantly negative correlation between FEV1%pred and the R5, R5-R20, and Fres, while a positive correlation between FEV1%pred and the X5. COPD patients had increased R5, R5-R20, and Fres, while decreased X5. The severity of bronchial obstruction found by impulse oscillometry correlated well the spirometric assessment. IOS parameters, R5, R5-R20, X5 and Fres may be useful for predictions and evaluations for COPD patients, and in initial stage the predictive value could be better. In particular, the R5-R20 and Fres have clearly the best predictive value for COPD. The IOS is a simple to perform test that is complementary to spirometry, and especially in elderly people it may be essential for functional examination of COPD patients.
2.Introduction
3.Materials and Methods
3.1.Subjects
3.2.Spirometry and Impulse Oscillometry (IOS)
3.3.Statistical Analysis
4.Results
4.1.Baseline Characteristics
4.2.Correlations Between The Severity of Airway Obstruction (FEV1%pred) and IOS Measurements
4.3.Contribution of Peripheral Resistance (R5-R20) To the Total Airway Resistance (R5)
4.4.Receiver Operating Characteristic (ROC) Curves Were Constructed to Evaluate the Diagnostic Ability of COPD
5.Discussion
6.Conclusions
7.Acknowledgments
8.References
Keywords
Lung function; Spirometry; Impulse oscillometry; Chronic obstructive pulmonary disease.
Introduction
Spirometry is a standard, objective lung function test for diagnosis of airflow limitation in chronic obstructive pulmonary disease (COPD) in accordance with the Global Initiative of Obstructive Lung Disease classification [1]. The essential diagnostic parameter for airway obstruction in COPD is a ratio of forced expiratory volume in 1 s to forced vital capacity FEV1/FVC of less than 0.70. The measurement of FEV1 allows assessing the severity of airway obstruction in COPD patients [2]. Spirometry is highly dependent on the performance technique, as the maximal inspiration and forced expiratory maneuver require the patient’s active cooperation [3].
Impulse oscillometry (IOS) measures both small and large airways resistance and resonance capacitance of the lung. Its main advantage is its ability to perform these measurements in a noninvasive, relatively effort independent, and minimally intrusive manner during spontaneous normal tidal breathing. In contrast to traditional spirometry, impulse oscillometry or IOS traces its findings independent of age, height, weight or gender [4]. In addition, IOS can also detect distal airways disorders that are not measured by spirometry [5]. Moreover, the IOS enables an assessment of total resistance (R5), proximal resistance (R20) and distal capacitive reactance (X5), as well as to calculate peripheral resistance (R5-R20) and resonance frequency (Fres) [6, 7]. Thus, IOS is considered as complementary to spirometry. This method can especially be recommended to elderly patients with physical and mental limitations or with poor pulmonary function, who may have difficulty in successfully performing spirometry [8]. The aim of this study was to compare IOS and spirometry in the assessment of airway obstruction in elderly COPD patients.
Materials and Methods
The study protocol involving patients was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University in Nanjing, China, and each participant recruited gave informed consent. The study was conducted in 141 stable COPD patients and 126 healthy subjects with normal spirometry as a control group. All study subjects were more than or equal to 60 years old. COPD was diagnosed in accordance with Global Initiative for Chronic Obstructive Lung Disease guidelines [1].
Spirometry and IOS measurements were evaluated after receiving 400 μg of short-acting beta2-agonist (salbutamol), according to ERS/ATS recommendations [9]. Flow-volume spirometric assessments included FEV1/FVC (FEV1%FVC), FEV1 (FEV1%pred) and FVC (FVC%pred). The spirometric criterion for airflow limitation was a fixed ratio of FEV1/FVC<0.70. Classification of airflow limitation severity was based on postbronchodilator FEV1%pred value according to GOLD standardizations [1]. The patients were stratified according to the severity of airway obstruction: mild (FEV1≥80%pred), moderate (50 %≤FEV1<80%pred), severe (30 %≤FEV1<50%pred), and very severe (FEV1<30%pred). IOS measurements included: total respiratory resistance at 5 Hz (R5) comprising extrathoracic, central, and peripheral airways; proximal resistance at 20 Hz (R20) comprising mainly extrathoracic and central airways; peripheral resistance at 5 Hz minus that at 20 Hz (R5-R20); distal capacitive reactance at 5 Hz (X5) comprising elastic lung and thorax components; resonance frequency (Fres) was determined as frequency where the reactance equals zero.
The oscillometric values of R5, R20, R5-R20, X5 and Fres were correlated with the FEV1%pred results. Data are given as mean ± standard deviation (SD). The relationship between pulmonary function parameters was assessed with Pearson’s correlation. Receiver operating characteristics (ROC) curve analysis was performed to evaluate the diagnostic value of COPD. The discriminative power of the various parameters studied was determined by means of ROC curves: the area under the curve (AUC), sensitivity and specificity. The ROC curves with AUC were plotted to demonstrate sensitivity and speci-ficity of the evaluated IOS. P-value < 0.05 was considered significant. Statistical analyses were performed using IBM SPSS statistics, version 19.0.
Results
The A total of 267 participants were enrolled into this study.Among 267 subjects, 141 were diagnosed with COPD (M/F-113/28; mean age of 76±7 years) and 126 healthy subjects (M/F-90/36; mean age of 72±7 years) with normal spirometry (Table 1). The patients were stratified according to the severity of airway obstruction: Mild (M/F, 44/10), Moderate (M/F, 46/12), Severe (M/F, 19/4) and Very severe (M/F, 4/2). The general characteristics of the study group showed the subjects in our study are elderly, and the mean BMI was normal at each group (Table 1). The IOS measurements performed in the course of COPD, confirmed the increases in total respiratory resistance (R5), peripheral resistance (R5-R20) and resonance frequency (Fres), and a decrease in negative reactance (X5) at all stages of airway obstruction (Table 1). This trend is increasingly obvious with increasing airway obstruction (Table 1).
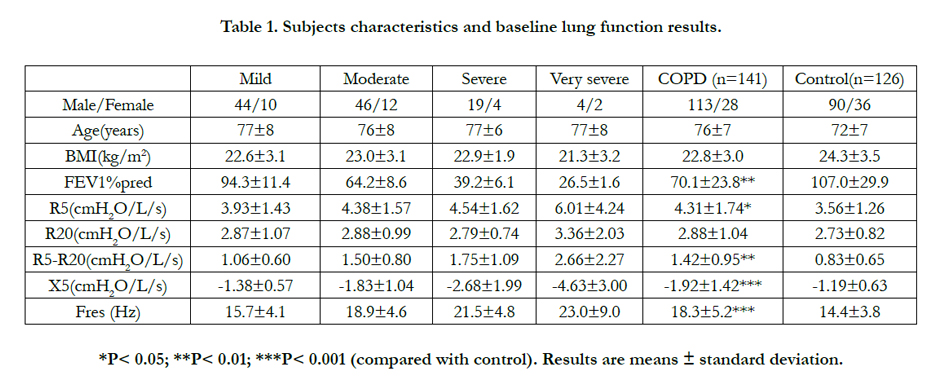

Table 1. Subjects characteristics and baseline lung function results.
The oscillometric measurements worsened with a higher degree of obstruction as assessed by spirometry (lower FEV1%pred). A negative correlation between the severity of airway obstruction and total respiratory resistance (R5) was significant (r = -0.264, p = 0.002) (Table 2, Figure 1a). There was no correlation between the airway obstruction and proximal resistance (R20) (r = -0.055, p = 0.517). The comparative evaluation of peripheral resistance (R5-R20) revealed a negative correlation with the severity of airflow limitation (r = -0.424, p = 0.000) (Table 2, Figure 1b). A positive correlation between the stage of airway obstruction and distal capacitive reactance (X5) was significant as well (r = 0.484, p = 0.000) (Table 2, Figure 1c). Meanwhile, the comparative evaluation of resonance frequency (Fres) revealed a negative correlation with the severity of airflow limitation (r = -0.509, p = 0.000) (Table 2, Figure 1d). What’s more, when we stratified the patients according to the severity of airway obstruction, we found some interesting results as follow: the comparative evaluation of R5- R20 revealed a negative correlation with the mild and moderate group (r = -0.313, p = 0.021; r = -0.301, p = 0.022); a positive correlation between the mild and moderate group and X5 was significant as well (r = 0.272, p = 0.047; r = 0.298, p = 0.023); the comparative evaluation of Fres revealed a negative correlation with the mild and moderate group (r = -0.355, p = 0.008; r = -0.290, p = 0.027). In addition, we found that a negative correlation between the severe group and R20 (r= -0.448, p= 0.032), and a positive correlation between the severe group and X5 (r= 0.436, p= 0.038). In groups other than mentioned above, no significant correlations were found (Table 2).
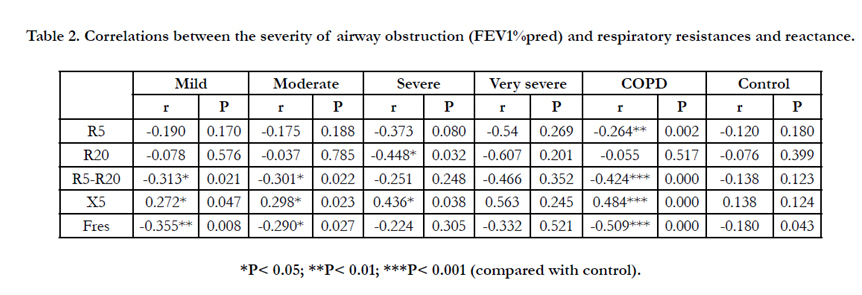
Table 2. Correlations between the severity of airway obstruction (FEV1%pred) and respiratory resistances and reactance.
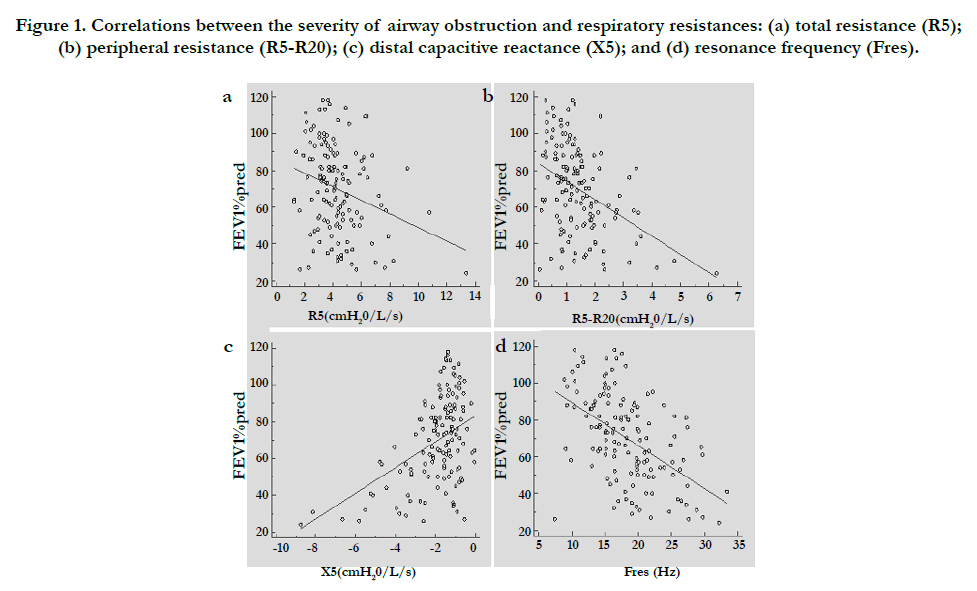
Figure 1. Correlations between the severity of airway obstruction and respiratory resistances: (a) total resistance (R5); (b) peripheral resistance (R5-R20); (c) distal capacitive reactance (X5); and (d) resonance frequency (Fres).
The contribution of peripheral resistance (R5-R20) to the total resistance (R5) depends on the severity of airway obstruction. The peripheral resistance was 23.3 % in the control group and its share increased in COPD patients accompany with increasing airway obstruction, amounting to 26.9 % in mild, 34.2 % in moderate, 38.6 % in severe, and 44.2 % in very severe obstruction (Figure 2).
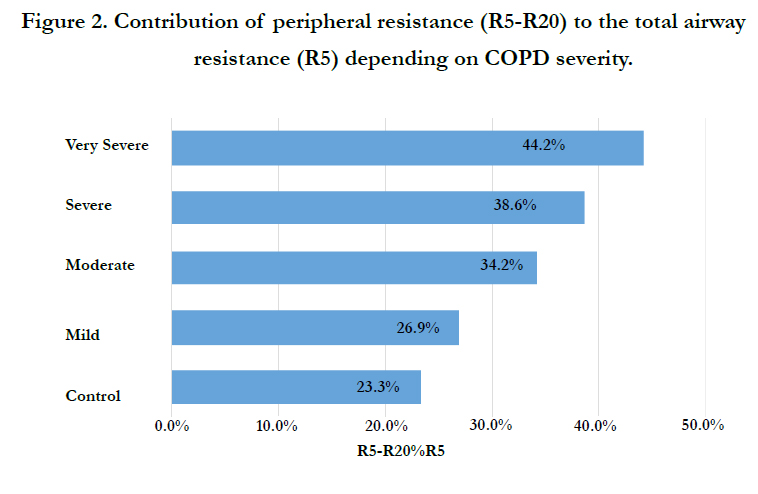
Figure 2. Contribution of peripheral resistance (R5-R20) to the total airway resistance (R5) depending on COPD severity.
ROC curves were constructed for each of the IOS measurements (Table 3 and Figure 3). For 126 normal subjects, they were just negative controls when established the optimal cut-off values for IOS parameters in ROC curves to diagnose COPD. Overall, all IOS measurements involved are correlated with COPD. In particular, R5, R5-R20, X5 and Fres have been found to be significantly correlated with COPD. The R5 had AUC of 0.661 and produced a sensitivity of 55.32% and a specificity of 75.4% for the diagnosis of COPD. The R5-R20 had AUC of 0.724 and produced a sensitivity of 78.72% and a specificity of 61.9% for the diagnosis of COPD. The X5 had AUC of 0.682 and produced a sensitivity of 60.99% and a specificity of 71.43% for the diagnosis of COPD. The Fres had AUC of 0.733 and produced a sensitivity of 64.54% and a specificity of 75.4% for the diagnosis of COPD. IOS parameters had predictive effects if AUC is higher than 0.7. Diagnostic performance of IOS parameters were shown in Table 3 and Figure 3. Thus, R5, R5-R20, X5 and Fres are correlated better with COPD. The R5-R20 and Fres have clearly the best predictive value for COPD.
Table 2. Correlations between the severity of airway obstruction (FEV1%pred) and respiratory resistances and reactance.
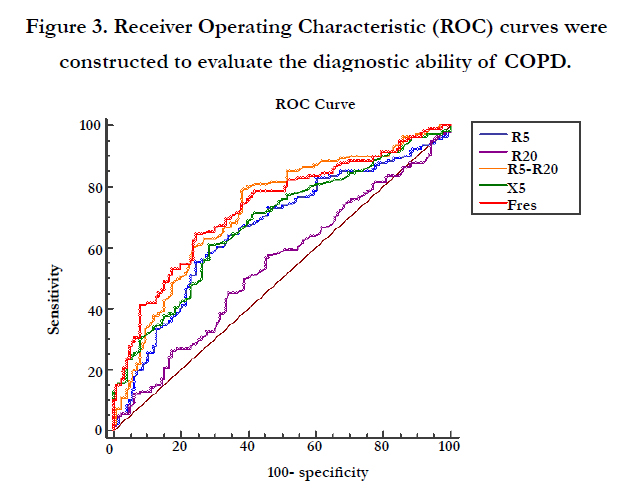
Figure 3. Receiver Operating Characteristic (ROC) curves were constructed to evaluate the diagnostic ability of COPD.
Discussion
Difficulties associated with the proper performance of respiratory maneuvers by elderly patients or patients at advanced stages of COPD, limit the use of spirometry in the assessment of lung function. In addition, spirometry measures mainly the proximal respiratory airflow, while COPD is notably a disease of peripheral airways [1, 6]. However, spirometry is high repeatability of measurements expressed by coefficients of variations [10]. Intriguingly, IOS can be a complementary method to conventional pulmonary function testing and, in selected cases, the method of choice in the evaluation of functional disorders in patients with COPD [11]. Additionally, there is a renewed interest in the IOS because of its non invasiveness and potential ability to distinguish a small from larger airway disease [2]. The repeatability of IOS measurements is lower than that of spirometry, and when expressed by coefficients of variations it does not usually exceed 20 % in obstructive diseases [12].
General assessment of COPD patients in the present study shows that the older age and lower BMI correlated with increasing airway obstruction, although the mean BMI was within the normal range at each stage of the disease. The mean BMI significantly goes down with COPD worsening [13]. It has been determined that the FEV1 alone is not a good diagnostic and prognostic measure of COPD, since it does not represent the whole of a respiratory disorder [6]. However, FEV1 complemented by IOS in the assessment of airflow limitation may become a measurement of components of airway resistance (R5). The present study shows the contribution of peripheral resistance (R5-R20) to total resistance (R5) depending on the stage of obstruction. Increased negative values of distal capacitive reactance (X5) were also found and they were correlated with increasing airflow limitation. The present study also shows negative correlations between the severity of airway obstruction (FEV1%pred) and the R5, R5-R20, and Fres of oscillometric measurements, while positive correlation between FEV1%pred and X5. However, correlation between FEV1%pred and R20 is insignificant. There were similar findings in other studies [7, 14, 15]. Other research suggested that IOS should be recommended for detecting respiratory abnormalities in COPD earlier than spirometry [16]. Moreover, it has been established that pulmonary function tests performed in tandem are more sensitive in detecting airflow limitation in COPD than IOS used separately, but have the same specificity in excluding bronchial obstruction [6]. Anderson et al., found that the IOS is useful for detecting airway disorders in COPD patients, but does not provide a link between symptoms assessed by the Medical Research Council Dyspnea Score and pulmonary function measurements [17].
Small airways are considered the major sites of airflow limitation in patients with COPD. However, the understanding of the exact role of small airway dysfunction in the clinical features and progression of the disease is still limited. One of the reasons is that, though spirometry is the gold standard to diagnose and manage COPD, there is little agreement on the most useful lung function parameter to evaluate the small airways [18, 19]. However, the forced oscillation technique has been successfully used as a measure of the airway resistance heterogeneity and gas trapping [20]. Notably, IOS has been used to exhaustively investigate small airway dysfunction in patients with asthma [21, 22]. In patients with COPD, IOS has been recently used to measure both proximal and peripheral airway resistance [5, 23, 24]. In our study, we found that R5-R20, X5 and Fres were all significantly correlated with the severity of airway obstruction (FEV1%pred), especially in mild and moderate group. This indicates that IOS parameter can evaluate small airway situation in COPD patients, and in COPD initial stage the predictive value could be better.
In the present study, 267 participants were categorized in two groups. After inhaling salbutamol, IOS and spirometry measurement was detected by devices. Compared with the control group (normal subjects), the results showed that IOS was useful to diagnose COPD. In IOS parameters, R5, R5-R20, X5 and Fres are correlated better with COPD. In particular, the R5-R20 and Fres have clearly the best predictive value for COPD. And these IOS parameters of sensitivity and specificity are good for COPD. We found that peripheral airway resistance and airway elastic resistance increased in patients with COPD, and Li et al., reported similar findings in their study [25].
Conclusions
COPD patients have increased total and peripheral airway resistance, and decreased negative reactance. The severity of bronchial obstruction assessed by spirometry (FEV1%pred) correlates with the measures obtained from an oscillometric method. IOS parameters, R5, R5-R20, X5 and Fres may be useful for predictions and evaluations for COPD patients, and in initial stage the predictive value could be better. Notably, R5-R20 and Fres have clearly the best predictive value for COPD. The IOS is a simple to perform test that is complementary to spirometry, and especially in elderly people it may be essential for functional examination of COPD patients.
Acknowledgments
This study was funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions (Jiangsu, China), and also supported by grants from the International Science & Technology Cooperation Program of China (No. 2014DFA31940), the National Natural Science Foundation of China (Beijing, China; Nos. 81572259, 30971320, 81272602 and 81302011), and the Cadre Health Care Research Project of Jiangsu Province (No. BJ14008).
References
- Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, et al. (2013) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 187(4): 347-365.
- Cooper CB (2005) Assessment of pulmonary function in COPD. Semin Respir Crit Care Med 26(2): 246-252.
- Kubota M, Shirai G, Nakamori T, Kokubo K, Masuda M, et al., (2009) Low frequency oscillometry parameters in COPD patients are less variable during inspiration than during expiration. Respir Physiol Neurobiol. 166(2): 73-79.
- Goldman MD, Saadeh C, Ross D (2005) Clinical applications of forced oscillation to assess peripheral airway function. Respir Physiol Neurobiol. 148(2): 179-194.
- Crim C, Celli B, Edwards LD, Wouters E, Coxson HO, et al., (2011) Respiratory system impedance with impulse oscillometry in healthy and COPD subjects: ECLIPSE baseline results. Respir Med. 105(7): 1069-1078.
- Jarenbäck L, Ankerst J, Bjermer L, Tufvesson E (2013) Flow-volume parameters in COPD related to extended measurements of lung volume, diffusion, and resistance. Pulm Med 2013:782052.
- Kanda S, Fujimoto K, Kamatsu Y, Yasuo M, Hanaoka M, et al., (2010) Evaluation of respiratory impedance in asthma and COPD by an impulse oscillation system. Intern Med. 49(1): 23-30.
- Janssens JP, Nguyen MC, Hrrmann FR, Michel JP (2001) Diagnostic value of respiratory impedance measurements in elderly subjects. Respir Med. 95(5): 415-422.
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, et al., (2005) Interpretative strategies for lung function tests. Eur Respir J. 26(5): 948-968.
- Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, et al., (2005) General considerations for lung function testing. Eur Respir J. 26(1): 153-161.
- Schulz H, Flexeder C, Behr J, Heier M, Holle R, et al., (2013) Reference values of impulse oscillometric lung function indices in adults of advanced age. PLoS One. 8(5):e63366.
- Oostveen E, MacLeod D, Lorino H, Farré R, Hantos Z, et al., (2003) The forced oscillation technique in clinical practice; methodology, recommendations and future developments. Eur Respir J. 22(6): 1026-1041.
- De S (2012) Body mass index among patient with chronic obstructive pulmonary diseases. Indian J Physiol Pharmacol. 56(4): 353-358.
- Piorunek T, Kostrzewska M, Cofta S, Batura-Gabryel H, Andrzejczak P, et al., (2015) Impulse oscillometry in the diagnosis of airway resistance in chronic obstructive pulmonary disease. Adv Exp Med Biol. 838: 47-52.
- Qi GS, Zhou ZC, Gu WC, Xi F, Wu H, et al., (2013) Detection of the airway obstruction stage in asthma using impulse oscillometry system. J Asthma. 50(1):45-51.
- Winkler J, Hegert-Winkler A, Wirtz H, Schauer J, Kahn T, et al., (2009) Impulse oscillometry in the diagnosis of the severity of obstructive pulmonary disease. Pneumologie. 63(5):266-275.
- Anderson WJ, Lipworth BJ (2012) Relationships between impulse oscillometry, spirometry and dyspnoea in COPD. J R Coll Physicians Edinb. 42(2): 111-115.
- Stewart JI, Criner GJ (2013) The small airways in chronic obstructive pulmo- nary disease: pathology and effects on disease progression and survival. Curr Opin Pulm Med. 19(2):109-115.
- Burgel PR (2011) The role of small airways in obstructive airway diseases. Eur Respir Rev. 20 (119): 23-33.
- King GG, Downie SR, Verbanck S, Thorpe CW, Berend N, et al., (2005) Effects of methacholine on small airway function measured by forced oscillation technique and multiple breath nitrogen washout in normal subjects. Respir Physiol Neurobiol. 148(1-2): 165-177.
- van der Wiel E, Postma DS, van der Molen T, Schiphof-Godart L, Ten Hacken NH, et al., (2014) Effects of small airway dysfunction on the clinical expression of asthma: a focus on asthma symptoms and bronchial hyperresponsiveness. Allergy. 69(12): 1681-1688.
- Alfieri V, Aiello M, Pisi R, Tzani P, Mariani E, et al., (2014) Small airway dysfunction is associated to excessive bronchoconstriction in asthmatic patients. Respir Res. 15: 86.
- Frantz S, Nihlén U, Dencker M, Engström G, Löfdahl CG, et al., (2012) Impulse oscillometry may be of value in detecting early manifestations of COPD. Respir Med. 106(8): 1116-1123.
- Mineshita M, Shikama Y, Nakajima H, Nishihira R, Komatsu S, et al., (2014) The application of impulse oscillation system for the evaluation of treatment effects in patients with COPD. Respir Physiol Neurobiol. 202:1-5.
- Li Y, Chen Y, Wang P (2015) Application of impulse oscillometry and bronchial dilation test for analysis in patients with asthma and chronic obstructive pulmonary disease. Int J Clin Exp Med. 8(1): 1271-1275.





