Physiological Effect of Chromium Exposure: A Review
Teklay A
Department of BioMedical Sciences, Physiology Team, College of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia.
*Corresponding Author
Abraha Teklay,
Department of BioMedical Sciences, Physiology Team,
College of Medicine and Health sciences, Adigrat University,
Adigrat, Ethiopia.
E-mail: abrahateklay@yahoo.com
Received: May 05, 2016; Accepted: June 02, 2016; Published: June 03, 2016
Citation: Teklay A (2016) Physiological Effect of Chromium Exposure: A Review. Int J Food Sci Nutr Diet, S7:001, 1-11. doi: dx.doi.org/10.19070/2326-3350-SI07001
Copyright: Teklay A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Human exposure to metals is common due to their wide use in industry, and environmental persistence. The heaviest metal exposures occurred in the workplace or in environmental settings in close proximity to industrial sources. Chromium is one of the heaviest metals. Although chromium relative atomic mass is 51.996g it may found in 0, +2, +3 and +6 forms. Metal chromium (0) is used in steel production, whereas chromium (VI) and chromium (III) are used for chrome plating, dyes and pigments, leather tanning, and wood preserving. Divalent chromium (Cr2+) is a strong reductant. Chromium (VI) compounds are more toxic than chromium (III) compounds. Chromium (III) occurs naturally in the environment. The daily intake of chromium from food, air, and water is estimated, respectively, as 60, < 0.2-0.6, and < 4.0μg. Chromium enters the air, water and soil in the chromium(III) and chromium(VI) form through natural processes and human activities. A possible source of chromium exposure to the general public is waste dumps for chromate producing using local air or water pollution. Chromium compounds (chromates, dichromates and chromic acid) pose the most significant health hazards. Generally the health problems that are caused by chromium exposure are:- It can cause allergic reactions, such as skin rash; nose irritations and nosebleeds; Upset stomachs and ulcers; Respiratory problems such as respiratory tract irritant to the nose, throat and lungs; Weakened immune systems; Kidney and liver damage; Alteration of genetic material; Lung cancer and Death. The physiological effect of chromium exposure is not restricted to these effect only; but also, it affects other many physiological parameters including of:- Skin effects; Cardiovascular effects; Hematological effects; Reproductive and developmental effects; Gastrointestinal effects; Ocular effects; Neurological effects and so on.
2.Introduction
2.1 What are the health hazards of chromium exposures
3.Literature Review
3.1 Respiratory System Effects
3.2 Skin Effects
3.3 Cardiovascular system effects
3.4 Renal system effects
3.5 Hematological effects
3.6 Reproductive and developmental effects
3.7 Gastrointestinal system effects
3.6 Hepatic effects
3.7 Other Effects
4.Conclusion
5.Acknowledgements
6.References
Keywords
Physiological Effect; Chromium Exposure.
Introduction
Human exposure to metals is common due to their ubiquity, wide use in industry, and environmental persistence. The heaviest metal exposures are occurred in the workplace or in environmental settings in close proximity to industrial sources. Chromium is one of the heaviest metals. Chromium is a lustrous, brittle, hard, multivalent metallic element; resistant to corrosion and tarnishing. It is a transition metal with an atomic weight of 52. Chromium is unstable in oxygen, it immediately produces a thin oxide layer that is impermeable to oxygen and protects the metal below.
Although chromium may theoretically occur in all oxidation states, it is most often found in 0, +2, +3 and +6. Elemental chromium (0) is not naturally present in the earth crust and is biologically inert. Almost all naturally found Cr is trivalent while hexavalent Cr is mostly of industrial origin. Most Cr compounds are halides, oxides or sulphides [12, 19, 20]. Divalent chromium (Cr2+) is a strong reductant; the form is readily oxidised when in contact with air, producing Cr3+. This explains why divalent Cr is not available in biological systems. Trivalent chromium (Cr3+) is the most stable oxidation state in which Cr is found in living organisms. It does not have the capacity to cross cell membranes easily and has a low reactivity, which is the most significant biological feature distinguishing it from Cr6+. Hexavalent chromium (Cr6+) is the second most stable form and a strong oxidising agent, especially in acidic media. Hexavalent chromium is bound to oxygen as chromate (CrO4 2–) or dichromate (Cr2O7 2–) with a strong oxidative capacity. This form of Cr crosses biological membranes easily, reacting with protein components and nucleic acids inside the cell while being deoxygenated to Cr3+. The reaction with genetic matter provides for the carcinogenic properties of Cr6+ [12, 19].
Chromite ores are used as refractory bricks; chromium (0) metal is used as ferrochromium in steel and other alloy production; while chromium (III) and chromium (VI) chemicals are used for chrome plating, the manufacture of dyes and pigments, leather tanning, and wood preserving [4, 9, 20].
Both trivalent and hexavalent chromium are found in nature, but the trivalent is the more common form. Chromium in biological materials is probably always trivalent. In the biologic system there is very low chance of conversion of trivalent chromium to hexavalent chromium and it is the hexavalent chromium that crosses the cell membrane and becomes reduced to trivalent chromium, which is then involved in various cellular reactions [2]. The site in the cell for this conversion (hexavalent form to the trivalent form) has been suggested to be the plasma membrane, the endoplasmic reticulum, the mitochondria or the cell nucleus. The biological effects of the hexavalent form may thus either be related to the reduction process or to the subsequent binding of the trivalent chromium to macromolecules, or possibly to both [2, 4].
Trivalent chromium complexes with a number of ligands within the cell. High concentration of chromium is normally found in nucleic acids. Its function, if any, is not known, but a stabilizing effect of chromium on RNA has been demonstrated. Chromium exposure to the general public has important health consequences because of its skin sensitizing effect. Chromium is among the most common sensitizers in allergic eczema. The daily intake of chromium from food, air, and water is estimated, respectively, as 60, < 0.2-0.6, and < 4.0μg [2].
The potential industrial sources of chromium release or Chromium enters the air, water and soil in the chromium (III) and chromium (VI) form through natural processes and human activities. The main human activities that increase the concentrations of chromium (III) are steal, leather and textile manufacturing. The main human activities that increase chromium (VI) concentrations are chemical, leather and textile manufacturing, electro painting and other chromium (VI) applications in the industry [27]. These applications will mainly increase concentrations of chromium in water. Through coal combustion (coal ash from electric utilities and other industries) chromium will also end up in air and through waste disposal chromium will end up in soils [4]. In chromate production, high exposures to chromium (III) were reported for the dry end mixing and roasting operations (> 1 mg/m3), while high levels of chromium (VI) predominated in the end product filtering and shipping areas (0.08-8.8 mg/m3). High levels of hexavalent chromium (> 1mg/m3) have also been found in chrome plating and in some types of chrome steel welding operations. In ferrochromium operations, chromium (III) predominates, but chromium (VI) has also been recovered at low levels, while tanning operations involve only chromium (III) exposures [9, 10].
A possible source of chromium exposure to the general public is waste dumps for chromate producing plants using local air or water pollution. Exposure to chromium occurs from ingesting contaminated food or drinking water or breathing contaminated workplace air. Generally People can be exposed to chromium through breathing in dust, fumes or mist; eating or swallowing it, through handling food when one have chromium dust on hands or through drinking and through skin contact with solutions or solids of chromium or chromium compounds [4].
The level of chromium in air and water is generally low. In drinking water the level of chromium is usually low as well, but contaminated well water may contain the dangerous chromium (IV). For most people eating food that contains chromium (III) is the main route of chromium uptake, as chromium (III) occurs naturally in many vegetables, fruits, meats, yeasts and grains. Various ways of food preparation and storage may alter the chromium contents of food. When food in stores in steel tanks or cans chromium concentrations may rise [4].
Chromium (VI) compounds (the hexavalent forms of chromium - chromates, dichromates and chromic acid) pose the most significant health hazards. Their toxicity varies with how soluble (how easily they dissolve) in water [13]. The least soluble compounds, such as lead chromates or barium chromate, are relatively less toxic because less hexavalent chromium is likely to be released into the body.
Single exposures to hexavalent chromium compounds can cause:-
- Irritation and inflammation of the nose and upper respiratory tract;
- Irritation of the skin with skin contact and for chromic acid,burns to the skin, possibly leading to ulcers;
- Eye damage from splashes.
Repeated exposure to hexavalent chromium compounds cancause:-
- Damage to the nose, including ulcers and holes in the flap of tissue separating the nostrils;
- Inflammation of the lungs;
- Allergic reactions in the skin and respiratory tract;
- Kidney damage;
- Cancer of the lung;
- Potential effects on reproduction, in both male fertility and the development of unborn babies;
Adverse effects of the hexavalent form on the skin may include ulcerations, dermatitis, and allergic skin reactions. Inhalation of hexavalent chromium compounds can result in ulceration and perforation of the mucous membranes of the nasal septum, irritation of the pharynx and larynx, asthmatic bronchitis, bronchospasms and edema. Respiratory symptoms may include coughing and wheezing, shortness of breath, and nasal itch [4]. The above chromium exposure effects and others would be discussed and therefore, the objectives of this paper would be: to review physiological and carcinogenic effects, associated with chromium exposure.
“All things are poison and nothing is without poison, only the dose makes something not a poison”
Paracelsus (1493-1541) Swiss physician and alchemist.
Literature Review
Chromium (VI) is a respiratory tract irritant to the nose, throat and lungs. Symptoms may include runny nose, sneezing, coughing, itching, and a burning sensation. Repeated or prolonged exposure can cause sores to develop in the nose and result in nosebleeds [4]. If the damage is severe, the nasal septum (wall separating the nasal passages) develops a whole (perforation). Some employees can become allergic to hexavalent chromium so that inhaling chromate compounds can cause asthma symptoms such as wheezing and shortness of breath. Sensitization resulting in an asthmatic response can result from Cr (VI) exposure. According to the literature, repeated or prolonged exposure can damage the mucous membranes of the nasal passages and cause ulcers to form [4,7].
Occupational exposures often include mixed exposure to both Cr (III) and Cr (VI) [5]. Human occupational experience clearly indicates that, when inhaled, chromium compounds are respiratory tract irritants, resulting in airway irritation, airway obstruction, and lung, nasal, or sinus cancer. Dose, exposure duration, and the specific compound involved can determine chromium's adverse health effects [4].
Pulmonary irritant effects following inhalation of chromium dust can include
- asthma,
- chronic bronchitis,
- chronic irritation,
- chronic pharyngitis,
- chronic rhinitis,
- congestion and hyperemia,
- polyps of the upper respiratory tract,
- tracheobronchitis, and
- ulceration of the nasal mucosa with possible septal perforation [7].
Radiographic analysis from several reports revealed enlargement of the hilar (relating to or located near a hilum) region and lymph nodes. Consistent associations have been found between employment in the chromium industries and significant risk for respiratory cancer. A delayed anaphylactoid reaction was reported in a male worker occupationally exposed to chromium vapors from Cr (VI) trioxide baths and chromium fumes from stainless steel welding. A subsequent inhalation challenge with sodium chromate resulted in a reaction including late-onset urticaria, angioedema, and bronchospasm accompanied by tripling of plasma histamine levels.
In addition to that, many cases of nasal mucosa injury (inflamed mucosa, ulcerated septum, and perforated septum) have been reported in workers exposed to Cr (VI) in chrome-plating plants and tanneries [3]. A study of 43 chrome-plating plants in Sweden, where workers were exposed almost exclusively to Cr (VI) acid, revealed that all workers with nasal mucosa ulceration or perforation were periodically exposed to at least 20 (μg/m3) when working near the plating baths. (The newest U.S. permissible exposure level in the workplace for chromates and chromic acid is 5μg/m3 as a ceiling). In another study also revealed that, the period of exposure for workers experiencing nasal mucosal ulceration varied from 5 months to 10 years. Another epidemiological study in U.S. workers found that the median time from date first employed to date of first diagnosis of nasal ulceration was less than a month; the median Cr (VI) concentration was similar to concentrations reported in the Swedish study [4, 7].
Not only that but also, the occupational exposure to Cr (III) has also been associated with respiratory effects. One man developed coughing, wheezing, and decreased forced volume after an inhalation exposure to a sample of Cr (III) sulfate. In an industrial hygiene survey of 60 ferrochromium workers exposed to Cr (III) and Cr (VI) (0.02-0.19 mg total chromium/m3) conducted in another study, appreciably higher incidences of subjective symptoms of coughing, wheezing, and dyspnea were reported. They added that, the respiratory system in animals is also a primary target for inhalation exposure to chromium. Histological examination of the lung tissue revealed alterations representing mild nonspecific irritation after exposure to 0.9 or 25 mg Cr (III) trichloride for 30 min.
An extensive epidemiological survey was conducted of housewives who lived in an area of Tokyo, Japan, in which contamination from chromium slag at a construction site was discovered. The exposed population reported a higher incidence of subjective complaints of nasal irritation than the control population of the study [3].
In another similar study Chromate dust and fumes of chromium trioxide have been reported to cause asthma. Chromates, among other exposure agents in chromium plating, welding, and ferrochromium production, have been connected with cases of occupational asthma or bronchitis. Mining dust in an underground chromite ore mine has also been reported to cause chronic bronchitis [11]. Obstructive effects on lung function have also been found among chromium workers [12]. In one study reduced forced vital capacity (FVC) and an increased prevalence of obstructive lung diseases were found among electro furnace workers in a ferrochromium plant. The author suggested that the effects were due to high levels of total dust, especially amorphous silica dust. According to the literature, nodular pneumoconiosis is another finding among workers in chromate production [12].
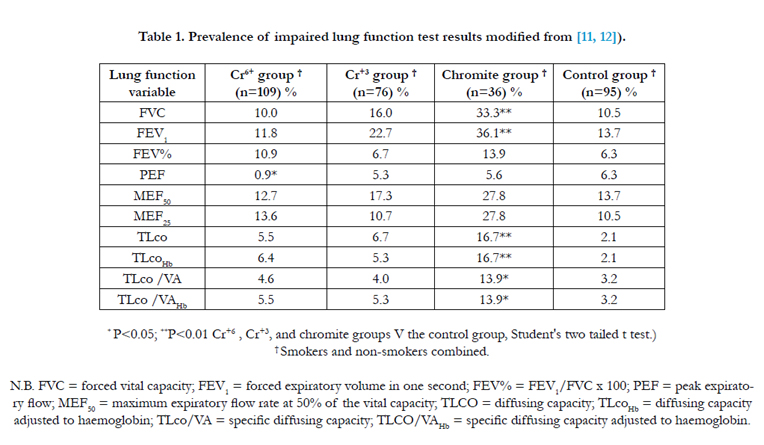
Moreover, in a study on respiratory symptoms among 60 ferrochromium workers in Norway pneumoconiosis was diagnosed from the radiographical examinations [12]. The production of phlegm was more frequent in the Cr+3 and chromite groups than in the other groups. Work related cough or dyspnoea was significantly more frequent in the Cr+6 (P = 0-041) and the Cr+3 (P = 0-033) groups than in the control group [11, 12]. In similar study, the author explained the occurrence of most of the respiratory symptoms; allergic diseases were associated with the occurrence of shortness of breath (dyspnoea) [11, 12].
Another similar study also shown that, the smokers in the chromite group had significantly lower FVC, FEV1, and diffusing capacity values than the smokers in the control group [12]. In this study, The percentages of the lung function test results that were below the predicted values were similar among the exposed groups, except for the chromite group, for which all the diffusing capacity variables and the FVC, FEV1, and MEF50 were significantly decreased (Table 1.) [11, 12].
In addition to that, the radiographic parenchymal abnormalities were found more often, but not significantly among the workers in the chromite groups [11]. The changes in the parietal and visceral pleura were also more frequent (not significantly) among the workers exposed to chromite [11, 12]. They also reported that, they had experienced the following symptoms during the years they were working for the chromite company: frequent cough (16.2%), production of phlegm (16.2%), shortness of breath (13.5%), rhinitis (35.1%), eye irritation (8.1%), dermatitis (18.9%), and various symptoms (headache, vertigo, fatigue, etc, 16.2%) [11,12].
Chromium (VI) compounds are not only powerful skin irritants but also can be corrosive. Contact with non-intact skin can also lead to chrome ulcers. These are small crusted skin sores with a rounded border. Ulcers can penetrate deep into soft tissue or become the site of secondary infections. They heal slowly and leave scars. Common sites for these ulcers include the nail root, knuckles and finger webs, back of the hands, and forearms. Some workers develop an allergic skin reaction, called allergic contact dermatitis. This occurs from handling liquids or solids containing hexavalent chromium. Once a worker becomes sensitized, contact with even small amounts can cause a serious skin rash [4].
Allergic contact dermatitis is long-lasting and more severe with repeated skin contact. The chrome sore begins as a pimple, forming an ulcer with raised hard edges. Ulcers may penetrate deep into soft tissue or becomes the site of secondary infection, but are not known to lead to cancer. The lesions heal slowly and may persist for months. Some workers develop an allergic reaction to chromium. Acute systemic and dermal allergic reactions have been observed in chromium sensitive individuals exposed to chromium via inhalation. No studies were located regarding systemic dermal effects in animals after inhalation exposure to chromium (VI) or chromium (III) compounds [14].
In the same study, the dermal exposure to chromium has been demonstrated to produce irritant and allergic contact dermatitis. Primary irritant dermatitis is related to the direct cytotoxic properties of chromium, while allergic contact dermatitis is an inflammatory response mediated by the immune system. Allergic contact dermatitis is a cell-mediated immune response that occurs in a two-step process. In the first step (induction), chromium is absorbed into the skin and triggers the next step - an immune response (sensitization). Sensitized individuals will exhibit an allergic dermatitis response when exposed to chromium above a threshold level. Localized erythematous or vesicular lesions at points of contact or generalized eczematous dermatitis should suggest sensitization [4, 14].
Chromium allergic dermatitis is characterized by symptoms of
- Dryness,
- Erythema, (Abnormal redness of the skin resulting from dilation of blood vessels)
- Fissuring, (Break into fissures or fine cracks)
- Papules, (A small inflamed elevation of skin that is nonsuppurative)
- Small vesicles and swelling [4].
The authors added that, solubility and pH appear to be the primary determinants of the capacity of individual chromium compounds to elicit an allergic response. The low solubility Cr (III) compounds are much less efficient contact allergens than Cr (VI). Penetration of the skin will cause painless erosive ulceration ("chrome holes") with delayed healing. The characteristic chrome sore begins as a papule, forming an ulcer with raised hard edges. Ulcers can penetrate deep into soft tissue or becomes the site of secondary infection, but are not known to lead to malignancy [6,14].
In addition to that, occupational exposure to Cr (VI) compounds has been associated with effects on the skin, nasal septum, and eardrum [7]. Chromium is one of the most common skin sensitizers and often causes skin sensitizing effect in the general public. A possible source of chromium exposure is waste dumps for chromate-producing plants causing local air or water pollution [4].
Information regarding cardiovascular effects in humans after inhalation exposure to chromium and its compounds is limited. Case reports of humans who died after ingesting Cr (VI) compounds have described cardiovascular effects as part of the sequelae leading to death [4].
The study by Wedeen and Qiant (1991) showed that, a 22 month old boy who ingested an unknown amount of sodium dichromate died of cardiopulmonary arrest. Autopsy revealed early hypoxic changes in the myocardium. A 35-year-old woman developed cardiovascular collapse and shock within a few hours following ingestion of 50 mL chromic acid [26]. A woman ingested 400ml of leather tanning solution containing 48grams of basic chromium sulphate (CrOHSO4). The patient died of cardiogenic shock, complicated by pancreatitis and gut mucosal necrosis and hemorrhage [4]. A 33-year-old male developed hypotension, ventricular arrhythmias, severe respiratory distress, and metabolic acidosis after ingesting an unknown amount of a liquid wood preservative containing chromium trioxide, arsenic pentoxide, and copper oxide [4, 26].
In another study, the cardiovascular function was studied in 230 middle aged workers involved in potassium dichromate production who had clinical manifestations of chromium poisoning (96 with respiratory effects and 134 with gastrointestinal disorders) and in a control group of 70 healthy workers of similar age. Both groups with clinical manifestations had changes in the bioelectric and mechanical activity of the myocardium as determined by electrocardiography, kinetocardiography, rheocardiography, and ballistocardiography. These changes were more pronounced in the workers with respiratory disorders due to chromium exposure than in the workers with chromium-induced gastrointestinal effects. The changes in the myocardium could be secondary to pulmonary effects and/or to a direct effect on the blood vessels and myocardium [26].
According to [26], the absence of reports regarding cardiovascular effects or disease due to chromium may not indicate the absence of an adverse cardiovascular effects but merely the absence of adequate clinical and epidemiological investigation.
Renal system effect is also another effect to chromium exposure. Kidney disease is often cited as an adverse effect of chromium [26]. Renal effects after inhalation or oral exposure to Cr (VI) compounds have been reported. Occupational exposure to Cr (III) does not appear to be associated with renal effects [3]. No renal impairment based on urinary albumin, retinol binding protein, and renal tubular antigens was found in 236 workers employed in the ferrochromium production industry [3].
Although glomerular injury has been noted in chromium workers, the predominant renal injury is tubular, with low doses acting specifically on the proximal convoluted tubules. Injury to the brush border membrane is a feature of chromate nephropathy. Severe poisoning can lead to acute tubular necrosis and acute renal failure. Low dose chronic Cr (VI) exposure typically results only in transient renal effects.
Elevated urinary Β2-microglobulin levels (an indicator of renal tubular damage) have been found in chrome platers, and higher levels have generally been observed in younger persons exposed to higher Cr (VI) concentrations.
In contrast to the paucity of evidence on chromium induced chronic renal disease, massive exposure to hexavalent chromium consistently causes acute tubular necrosis (ATN), clinically evident as a marked reduction in urine flow rate, if the patient survives for more than a few hours. ATN is characterized by the rapid onset of renal failure. Following heavy acute absorption, symptomatology is initially dominated by overwhelming pulmonary or gastrointestinal toxicity, depending on the route of exposure. In the syndrome of ATN, early oliguria (urine output less than 200 mL/day in adults) is followed by a polyuric phase (urine output exceeding 3 L/day), and subsequent gradual recovery of renal function over a few weeks. ATN caused by massive absorption of chromic acid and successful treatment by dialysis has been reported. Acute renal failure from accidental exposure to either trivalent or hexavalent chromium in the workplace is, however, distinctly rare [26]. Potassium dichromate produces necrosis in the convoluted portion of the proximal tubule [4].
Studies using radioactive Cr placed intratracheally in animals indicate chromium is selectively accumulated in the renal cortex at a 6 to 20 fold higher concentration than in red blood cells or liver [26]. Both trivalent and hexavalent chromium are accumulated up to 80 fold above the incubation medium concentration in the slice preparation by a process that appears to represent active (energy requiring) biologic transport. Renal cortical accumulation of chromate demonstrated by low resolution autoradiography appears to represent uptake in the convoluted portion of proximal tubules, the site of cellular necrosis. Although it is generally agreed that the trivalent form of chromium is less nephrotoxic than the hexavalent form, tubular necrosis and acute renal failure have been reported from both species of the metal.
In contrast to the trivalent form, hexavalent chromium is water soluble and readily penetrates cell membranes [4]. Absorption is less than 1% from the intestinal tract for both oxidation states. While the hexavalent form facilitates entry into the circulation and cell, cellular injury is believed to be initiated by intracellular protein binding of the trivalent form [26].
In another studies suggestive evidence that, chronic low dose exposure to chromium has adverse effects on the kidneys arises from the finding of low molecular weight (LMW) proteinuria in chromium workers. Excessive urinary excretion of Β2 microglobulin, a specific proximal tubule brush border protein (BB-50) and an extra-renal enzyme, retinol-binding protein, have been reported among some chrome platers and welders [4, 26].
Chromate induced ATN and tubular proteinuria, nevertheless, suggest that low level, long term exposure to chromium might produce chronic renal injury. Repeated minor tubular insults would be expected to eventually result in chronic interstitial nephritis. In contrast to glomerular disease, which is readily detected by simple tests for urinary albumin, interstitial nephritis is difficult to detect before the renal disease has become advanced, that is before more than two-thirds of kidney function is lost. At this relatively late state, there is sufficient reduction in the glomerular filtration rate to be detected by standard laboratory tests: elevation of the serum urea nitrogen and creatinine concentration [26]. Because of the long delay in appearance, the relatively low attack rate, the difficulty in detecting early interstitial nephritis, and the multifactorial nature of kidney disease, chronic renal disease caused by chromium is unlikely to be identified in the usual oneon- one physician patient encounter. Since chromium may accumulate in kidney tissue over many months, and the biological half life approximates 1 month, it may be possible to develop a chelation test to assess cumulative absorption comparable to the EDTA lead mobilization test that has proven so useful in identifying lead nephropathy. Moreover, the contribution of chromium to renal failure may only be evident when superimposed on other causes of renal injury such a lead nephropathy, hypertension, or diabetes mellitus or as a reduction in the renal reserve [26].
In another study they showed that, after rapid absorption of hexavalent chromic ions through the skin the kidney Organ damage can occur. While the skin lesions were relatively self limited, the patient manifested acute renal failure complicated with acute respiratory failure for a prolonged period. Serum creatinine level did not return to normal until 70 days after exposure. Chromium is mainly excreted through urine, with an initial half life of 2–3 days, followed by a terminal half life of about 1 month [4, 16].
They added that, although the patient developed prolonged acute renal failure, his condition gradually improved. On day 10, he was transferred to the general ward and no longer required hemofiltration, plasmapheresis, or therapy with DMPS and N-acetylcysteine. Acute renal failure was managed with hemodialysis until day 30. The Details of serial urine chromium and serum creatinine measurements are shown in (Figure 1.)[16].
To conclude, both trivalent and hexavalent chromium compounds are selectively accumulated in the proximal convoluted tubule where, in large dosage, they induce acute tubular necrosis following parenteral administration. Coupled with the finding of tubular proteinuria in chromium workers, there is reason to suspect that chromium contributes to the development of chronic renal failure [26].
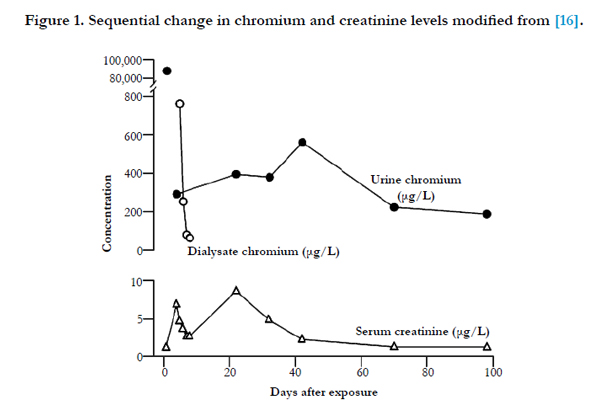
Figure 1. Sequential change in chromium and creatinine levels modified from [16].
Hematological effects is also another effect from chromium exposure. Blood is the most important tissues, in which changes in metabolic processes are going on, so abnormal alteration in blood parameters are the reliable indicators of toxic effects of drugs, chemicals and diseases [21]. The hematological evaluations of workers occupationally exposed to chromium compounds have yielded equivocal results. In one study ninety seven workers from a chromate plant were exposed to a mixture of insoluble chromite ore containing chromium (III) and soluble sodium chromate and dichromate; hematological evaluations revealed that, leukocytosis in 14.4% or leukopenia in 19.6% of the workers. Decreases in hemoglobin concentrations and slight increases in bleeding time were also observed [4].
In another similar studies, cases of hematological effects have been reported in humans after the ingestion of lethal or sublethal doses of Cr (VI) compounds. In a case of an 18-year-old woman who ingested a few grams of potassium dichromate, decreased hemoglobin content and hematocrit, and increased total white blood cell counts, reticulocyte counts, and plasma hemoglobin were found 4 days after ingestion. These effects were indicative of intravascular hemolysis. Laboratory analysis of a 35-year-old woman, who died 12 hours after ingesting 50 ml of pure chromic acid [25g Cr(VI)], revealed anemia (hemoglobin 56g/L, hematocrit 17%) and thrombocytopenia [21].
Results from hematological evaluations in rats were also equivocal. Hematological evaluations of rats exposed to sodium dichromate at 0.025–0.2 mg chromium(VI)/m3 for 28 or 90 days or 0.1 mg chromium(VI)/m3 for 18 months were unremarkable. However, increased WBC counts were found in rats exposed to 0.1mg chromium(VI)/m3 as sodium dichromate for 30 days and at 0.05 mg chromium(VI)/m3 for 90 days. The WBC counts were not increased 30 days postexposure. Rats exposed to 0.1 mg chromium/m3 as a 3:2 mixture of chromium (VI) trioxide and chromium(III) oxide for 18 months had increased RBC and WBC counts, hemoglobin content, and hematocrit. No changes in hematological parameters were observed in rats exposed to 15.5 mg
chromium (IV)/m3 as chromium dioxide for 2 years [21].
Another investigation on the effect of chromium in the normal mice dengue virus infection caused a significant reduction in the total leucocyte at day 4 (P < 0.05) and 8 (P < 0.01). The predominant cells in the blood remained lymphocytes [23]. According to them, Feeding chromium picolinate (CrP) had no effect on the RBC count, haemoglobin and MCV, whereas haematocrit concentration was significantly increased at 250mg/l dose of CrP [23].
In another study also revealed that, the concentration of hemoglobin decreased significantly (p<0.001) in the blood of fish exposed to combined heavy metals [25]. Heavy metals such as cadmium, chromium, Nickel and lead might alter the properties of hemoglobin by decreasing their affinity towards oxygen binding capacity rendering the erythrocytes more fragile and permeable, which probably results in cell swelling deformation and damage [25]. They demonstrated that, a significant decrease in RBC of common carp exposed to 5mg/L of combined heavy metals. Heavy metals increase the glucose content in blood, because of intensive glycogenolysis and the synthesis of glucose from extra hepatic tissue proteins and aminoacids [24, 25].
The study by Riaz et al., (2006) also shown that, Hemoglobin decreased at 3rd and 4th week and increased (highly significantly) from 5th to 9th week (Table 2.).
According the author, the total erythrocytes count is also increased highly significantly from 5th to 9th week (Table 3.) [21].
In addition to the above statements the authors added that, the total leukocyte count was increased highly significantly from 5th to 9th week (Table 4.) [21].
Not only that but also, the Packed Cell volume was increased highly significantly from 5th to 9th week (Table 5.) [21].
Generally the study shows that, Hb level, TEC and TLC were increased significantly after 5th, 6th and 7th week administrated chrome shavings in the feed of quail chicks. It also showed that, there was no significantly increase or decrease in packed cell volume. The chrome shaving did not cause the damage to the packed cell volume. The values however were the normal as compared to control group. So there was no significantly result in PCV. The increased in TEC, TLC and Hemoglobin contents were due to increased amount of chromium which accumulated in the body of quail chicks. Chromium caused toxicity and hence increased toxic levels in the body as disturbing the body normal functions [21, 24].
In another studies also shown that, the amounts of Hct, Hb, RBC, WBC, MCH, and MCHC significantly decreased (P<0.05) as a result of chronic chromium exposure, whereas blood albumin and glucose significantly (P<0.05) increased in the examined fish as opposed to the control. No significant differences (P > 0.05) were found between the Cr exposed fish and the control in the levels of Lym, Neu, MCV, IgM, and TP (Table 6.) [1, 24]. In addition to that, chronic chromium contamination increased glucose, neutrophils, and albumin concentrations [1].
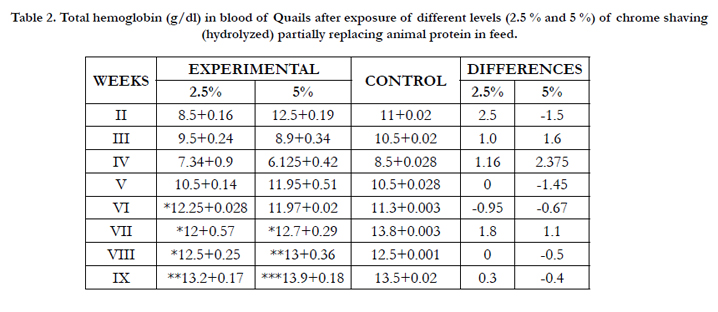

Table 2. Total hemoglobin (g/dl) in blood of Quails after exposure of different levels (2.5 % and 5 %) of chrome shaving (hydrolyzed) partially replacing animal protein in feed.
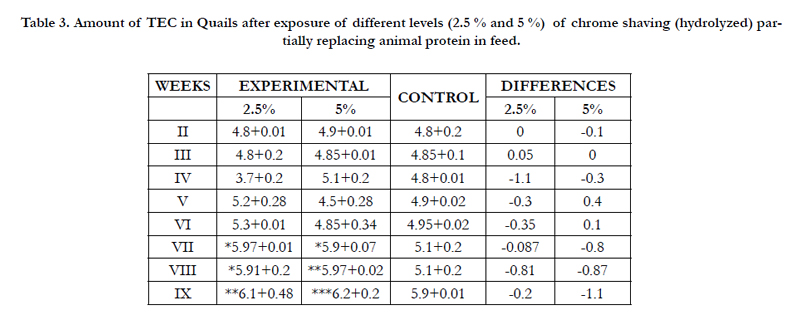
Table 3. Amount of TEC in Quails after exposure of different levels (2.5 % and 5 %) of chrome shaving (hydrolyzed) partially replacing animal protein in feed.
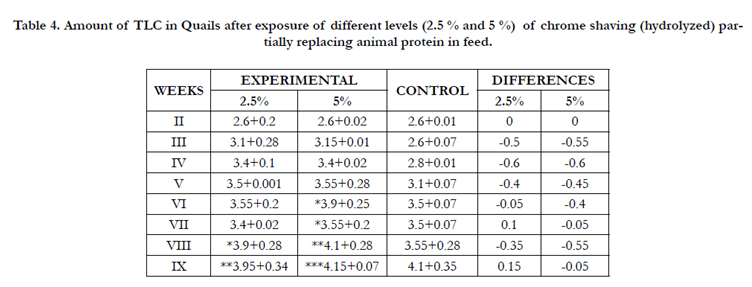
Table 4. Amount of TLC in Quails after exposure of different levels (2.5 % and 5 %) of chrome shaving (hydrolyzed) partially replacing animal protein in feed.
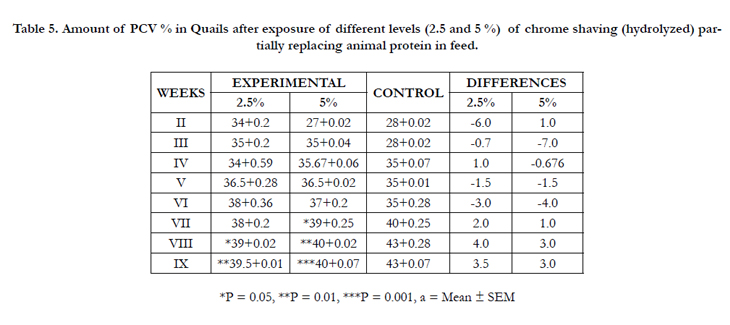
Table 5. Amount of PCV % in Quails after exposure of different levels (2.5 and 5 %) of chrome shaving (hydrolyzed) partially replacing animal protein in feed.
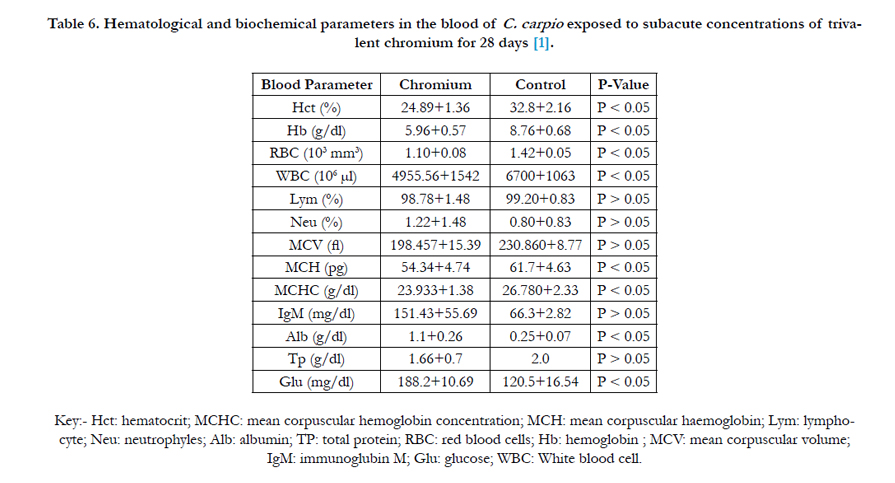
Table 6. Hematological and biochemical parameters in the blood of C. carpio exposed to subacute concentrations of trivalent chromium for 28 days [1].
Even though there were no more enough data were located regarding chromium in adverse human developmental effects, a few studies reported the effects of occupational exposure to mercury, manganese, chromium and boron on reproductive health in men [20]. However, the animal studies provide evidence that Cr (VI), after oral exposure, is a developmental toxicant in rats and mice [3]. The adverse developmental effects in animals include greater incidence of post implantation loss, decreased fetal body weight, reduced ossification, and decreased number of live fetuses. The study showed wives of stainless steel welders were at higher risk of spontaneous abortions [3].
Chromium (hexavalent compounds) was considered by the Developmental and Reproductive Toxicant Identification Committee (DARTIC) of the Office of Environmental Health Hazard Assessment's (OEHHA) Science Advisory Board at a public meeting held on November 20, 2008. At this meeting, the DARTIC determined that chromium (hexavalent compounds) was clearly shown through scientifically valid testing according to generally accepted principles to cause reproductive toxicity (developmental toxicity, male reproductive toxicity and female reproductive toxicity) [18]. Data on the male reproductive toxicity of chromium (hexavalent compounds), summarized by OEHHA (2009), include studies conducted in mice, rats, rabbits, and monkeys. Adverse effects included significant reductions in sperm counts, as well as in testes weights [20].
Another studies in laboratory animals shown that, high levels of hexavalent chromium cause testicular atrophy and decrease in sperm count. In human studies also, it has been found that exposure to chromium is significant in welders. Diminished sperm quality among welders has been demonstrated in a number of studies, but has not been definitively linked to exposure to chromium. As such, this profession is linked generally with occupational exposures affecting fertility. A biological theory exists stating a direct influence of lead and chromium on the structure of sperm, involving a partial exchange with zinc, which is an important ingredient of sperm that makes it heat resistant [20, 22].
In addition to that, exposure to chromium has some effect on human sperm as a significant positive correlation (r=0.301) was observed by [15]. More abnormal characteristics were found in the semen of exposed workers. According to Li et al., (2001), semen abnormalities correlated with the number of years of exposure to welding fumes containing nickel and chromium. The semen status of male workers occupationally exposed to hexavalent chromium (VI) was investigated. Sperm motility decreased for the exposed workers. Follicle stimulating hormone (FSH) in serum from the exposed workers was significantly higher than that from the control group [15, 20].
In another similar study, Feeding Cr (VI) to rats significantly reduced the epididymal sperm counts from epididymis in control group to epididymis at a CrO3 dose of 10mg/kg body weight and to epididymis at a CrO3 dose of 20mg/kg body weight. Exposure of rats to Cr (VI) also significantly increased the sperm abnormality from 2.75+/-0.06% in the control group to 6.68+/- 0.32% in the exposed group at a CrO3 dose of 10 mg/kg body and to 7.6+/-0.15% at a CrO3 dose of 20mg/kg body weight. In exposed rats, there was visible disruption in germ cell arrangement near the walls of the seminiferous tubules. The diameters of seminiferous tubules in exposed rats were smaller. These results suggest that occupational exposure to chromium (VI) leads to alteration of semen status and may affect the reproductive success of exposed workers [4, 15].
Another study was also reported that workers exposed to chromium (VI) had significantly higher serum follicle stimulating hormone concentration and lower sperm concentration and motility, seminal plasma zinc levels, lactate dehydrogenase (LDH), and LDH-C4, and significantly higher percentage of abnormal sperm than control workers. Blood chromium positively correlated with the percentage of abnormal sperm in the exposed workers Pizent et al., 2012). In a study of environmental chromium exposure, seminal chromium levels were not significantly different between fertile and infertile men. However, blood chromium was significantly associated with an increase in serum prolactin, and a non linear decrease in serum inhibin B. the literature added that, arsenic and chromium might adversely affect the male reproductive system [20].
OEHHA (2009) summarizes data on the female reproductive toxicity of chromium (hexavalent compounds) from studies in mice and rats performed by the drinking water route. All of the available studies in both species provided evidence for adverse effects on the female reproductive system at concentrations in drinking water ranging from 5ppm (ovarian alterations at the ultra structural level) to 1,000ppm (complete pregnancy failure in all exposed dams). Exposure to intermediate concentrations (500-750 ppm) was associated with effects including: lengthened estrous cycles; decreased mating and fertility indices; decreased numbers of corpora lutea, implantation sites, and live fetuses/litter; and increased frequencies of pre-and post-implantation loss, as well as resorption sites [4, 18].
Gastrointestinal effects have been associated with occupational exposure of humans to chromium compounds. In a report of two cases of acute exposure to "massive amounts" of chromium trioxide fumes, the patients complained of abdominal or substernal pain. For instance, in Health Hazard Evaluation of an electroplating facility in the United States, 5 of 11 workers reported symptoms of stomach pain, two of duodenal ulcer, one of gastritis, one of stomach cramps, and one of frequent indigestion. The workers were employed for an average of 7.5 years and were exposed to mean concentrations of 0.004mg chromium(VI)/m3 [4].
In another similar study of 97 workers from a chrome plant exposed to a mixture of insoluble chromite ore containing Cr (III) and soluble Cr (VI) as sodium chromate and dichromate, gastrointestinal radiography revealed that 10 of the workers had ulcer formation, and of these, six had hypertrophic gastritis. Nearly all of the workers breathed through the mouth while at work and swallowed the chromate dust, thereby directly exposing the gastrointestinal mucosa [17]. Most of these studies reporting gastrointestinal effects, however, did not compare the workers with appropriate controls [20].
Cases of gastrointestinal effects after oral exposure to Cr (VI) compounds have also been reported. In the study, a 14-year-old boy who died after ingesting 7.5 mg Cr (VI)/kg as potassium dichromate experienced abdominal pain and vomiting before death. Autopsy revealed gastrointestinal ulceration. In another study, a 44-year-old man died of gastrointestinal hemorrhage after ingesting 4.1mg Cr (VI)/kg as chromic acid solution [4, 17].
In a study in an otolaryngological examination of 77 employees of 8 chromium electroplating facilities in Czechoslovakia, where the mean level in the breathing zone above the plating baths was 0.414 mg chromium(VI)/m3, revealed 12 cases of chronic tonsillitis, 5 cases of chronic pharyngitis, and 32 cases of atrophy of the left larynx. In addition, in a survey of a facility engaged in chromate production in Italy where exposure concentrations were 0.01 mg chromium (VI)/m3, 15.4% of the 65 workers who worked in the production of dichromate and chromium trioxide for at least 1 year had duodenal ulcers and 9.2% had colitis. The ulcers were considered to be due to exposure to chromium. Gastric mucosa irritation leading to duodenal ulcer was found in 21 of 90 workers engaged in the production of chromium salts [20].
Although the gastrointestinal irritation and ulceration due to exposure to chromium (VI) in air could be due to a direct action of chromium (VI) on the gastrointestinal mucosa from swallowing chromium as a result of mouth breathing (or transfer via handto-mouth activity), other factors, such as stress and diet, can also cause gastrointestinal effects. In contrast to findings with chromium (VI) compounds, no indication was found that exposure to chromium (III) resulted in stomach disorders in workers employed in two factories that produced chromium (III) oxide or chromium (III) sulfate [20].
Information regarding gastrointestinal effects in animals after inhalation exposure to chromium or its compounds is limited. Histological examination of the stomachs of rats exposed to sodium dichromate dihydrate at 0.2 mg chromium (VI)/m3 for 28 or 90 days revealed no abnormalities. In mice exposed intermittently to 4.3 mg chromium (VI)/m3 as calcium chromate for 18 months, small ulcerations in the stomach and intestinal mucosa were reported to occur occasionally. No treatment related histopathological lesions were found in the stomach, large intestine, duodenum, jejunum, or ileum of rats chronically exposed to chromium dioxide at 15.5mg chromium(IV)/m3 [4].
Another effect of chromium exposure is hepatic effect. Cases of hepatic effects after oral exposure to Cr (VI) compounds have also been reported. Elevated liver enzyme levels were reported flowing ingestion of 150 mL solution containing 22.5g potassium dichrome. Hepatomegaly and hepatic failure [8] have also been noted in the cases of acute poisoning.
In another study showed that, Chromium (VI) has been reported to cause severe liver effects in four of five workers exposed to chromium trioxide in the chrome plating industry. Derangement of the cells in the liver, necrosis, lymphocytic and histiocytic infiltration and increases in Kupffer cells were reported. Abnormalities in tests for hepatic dysfunction included increases in sulfobromophthalein retention, gamma globulin, icterus, cephalin cholesterol flocculation, and thymol turbidity [8].
The hepatic effects observed in animals after inhalation exposure to chromium or its compounds were minimal and not considered to be adverse. Rats exposed to as much as 0.4 mg chromium (VI)/ m3 as sodium dichromate for 90 days did not have increased serum levels of alanine aminotransferase or alkaline phosphatase, cholesterol, creatinine, urea, or bilirubin [8]. Triglycerides and phospholipids were increased only in the 0.2 mg chromium (VI)/ m3 group exposed for 90 days. Chronic exposure of rats to 0.1 mg chromium(VI)/m3 as sodium dichromate, to 0.1 mg total chromium/m3 as a 3:2 mixture of chromium (VI) trioxide and chromium (III) oxide, or to 15.5 mg chromium (IV)/m3 as chromium dioxide did not cause adverse hepatic effects as assessed by histological examination and liver function tests [4].
However, according some literature, exposure to Cr (III) has not been found to cause any liver effects in workers employed in two factories that produced Cr(III) oxide or Cr(III) sulfate [8, 13].
Exposure to chromium not only affect the physiological parameters that we have been mentioned above but also affects other physiological parameters. For instance, higher incidences of subjective complaints of eye irritation were reported by [4]. Chromium (VI) is an eye irritant. Direct eye contact with chromic acid or chromate dusts can cause permanent eye damage. In addition, in a chrome plating plant where poor exhaust resulted in excessively high concentration of chromium trioxide fumes, workers experienced symptoms of dizziness, headache, and weakness when working over the chromate tanks [4].
In addition to the above effect, erosion and discoloration of the teeth may occur with Cr (VI) compounds exposure. Not only that but also, papillomas (A benign epithelial tumor forming a rounded mass) of the oral cavity and larynx have been reported in workers exposed to high air concentration of Cr (VI). Severe corneal injury may result from ocular contact with solid or concentrated solutions of chromic acid and other Cr (VI) compound [4]. However, no information was located regarding neurological effects in humans or animals after inhalation exposure to chromium (III) compounds or in animals after inhalation exposure to chromium (VI) compounds. No histopathological lesions were found in the brain, spinal cord, or nerve tissues of rats exposed to 15.5 mg chromium (IV)/m3 as chromium dioxide for 2 years.
Conclusion
From this review it can be concluded that as chromium is one of the heaviest metals, human exposure to heaviest metals is occurred in the workplace or in environmental settings in close proximity to industrial sources. Cr found in 0, +2, +3 and +6 forms. Elemental chromium (0) is not naturally present in the earth crust and is biologically inert; whereas all naturally found Cr is Cr3+ while Cr6+ is mostly of industrial origin. Cr3+ does not have the capacity to cross cell membranes and has a low reactivity however, the Cr6+ crosses biological membranes easily and reacts with protein components and nucleic acids inside the cell while being deoxygenated or reduced to Cr3+. Chromium enters the air, water and soil through natural processes and human activities. People can be exposed to chromium through breathing in dust, fumes or mist; through handling food eating or swallowing; drinking and skin contact with solutions or solids of chromium or chromium compounds. Their toxicity varies with how soluble in water. The least soluble compounds are relatively less toxic and therefore, most of the Cr toxicity is associated mainly with hexavalent chromium. The physiological effects of chromium exposure includes skin effects: such as allergic reactions, skin rash, skin irritants, dryness and swelling. It also includes respiratory system effects such as ulceration and perforation of nasal septum, irritation of the pharynx and larynx, asthmatic bronchitis, nose irritations, nose bleeding and lung cancer; Gastrointestinal effects: such as upset stomachs and ulcers; Renal effects such as acute tubular necrosis and chronic renal injury; Cardiovascular effects such as change in the myocardium alteration; Hepatic effects such as elevated liver enzymes and liver damages; Carcinogenic effects such as chromosome aberrations and sister chromatid exchanges; Genotoxic and mutagenic effects by altering genetic material; Hematological effects by affecting the blood parameters; Reproductive and developmental effects such as post implantation loss, decreased fetal body weight, reduced ossification, reductions in sperm counts or quality, sperm motility as well as in testes weight; Ocular effects and Neurological effects. In general physiological effects of chromium (Cr) exposure can lead to death.
Acknowledgements
I am very much indebted to my wife Nigsti Abadi for here consistent moral support and encouragement during my study.
Finally, I would like to thank, from the deep of my heart, to all my families and friends for their continuous moral support and encouragement in the course of this study.
References
- Abedi Z, Khalesi MK, Eskandari SK (2013) Biochemical and Hematological Profiles of Common Carp (Cyprinus Carpio) under Sublethal Effects of Trivalent Chromium. Iranian Journal of Toxicology 7(20): 782-792.
- Ahmad F, Javed MT, Sandhu MA, Kausar R (2004) Effects of higher levels of chromium and copper on broiler health and performance during the peak tropical summer season. VETERINARSKI ARHIV 74(5): 395-408.
- Agency for Toxic Substances and Disease Registry (ATSDR) 2000. Toxicological profile of chromium. Atlanta, Georgia, USA. 1-592.
- Agency for Toxic Substances and Disease Registry (ATSDR) 2011. Chromium Toxicity. Case Studies in Environmental Medicine (CSEM).USA. 1-67.
- United States Environmental Protection Agency(EPA) 1998. Toxicological review of trivalent chromium. USA.
- Geller R (2001) "Chromium." In: Clinical Environmental Health and Toxic Exposures. (2nd edn), Lippincott Williams & Wilkins, Philadelphia, PA.
- Gibb HJ, Lees PS, Pinsky PF, Rooney BC (2000) Lung cancer among workers in chromium chemical production. Am J Ind Med 38(2):115-126.
- Glaser U, Hochrainer D, Steinhoff D (1990) Investigation of irritating properties of inhaled Cr (VI) with possible influence on its carcinogenic action. In: Environmental hygiene II. Springer-Verlag, Berlin, Germany . 239- 245.
- Hayes RB (1997) The carcinogenicity of metals in humans. Cancer Causes Control 8(3): 371-385.
- Holmes AL, Wise SS, Wise JP (2008) Carcinogenicity of hexavalent chromium. Indian J Med Res 128(4): 353-372.
- Huvinen M, Uitti J, Oksa P, Palmroos P, Laippala P (2002) Respiratory health effects of long-term exposure to different chromium species in stainless steel production. Occupational Medicine 52(4): 203-212.
- Huvinen M, Uitti J, Zitting A, Roto P, Virkola K, et al. (1996) Respiratory health of workers exposed to low levels of chromium in stainless steel production. Occupational Occup Environ Med 53(11): 741-747.
- Korallus U, Ulm K, Steinmann-Steiner-Haldenstaett W (1993) Bronchial carcinoma mortality in the German chromate producing industry: the effects of process modification. Int Arch Occup Environ Health 65(3): 171-178.
- Lewis R (2004) Occupational Exposures: Metals. In: Current Occupational & Environmental Medicine. (3rd edn), Lange Medical Books/McGraw-Hill Companies, Inc. 439-441.
- Li H, Chen Q, Li S, Yao W, Li L, et al. (2001) Effect of Cr(VI) exposure on sperm quality: human and animal studies. Ann Occup Hyg 45(7): 505-511.
- Lin C, Wu M, Yang C, Ger J, Tsai W, et al. (2009) Acute Severe Chromium Poisoning After Dermal Exposure to Hexavalent Chromium. J Chin Med Assoc 72(4): 219–221.
- Mancuso TF (1997) Chromium as an industrial carcinogen: Part I. Am J Ind Med 31(2): 129-139.
- Office of Environmental Health Hazard Assessment (OEHHA) 2009. Evidence on the developmental and reproductive toxicity of chromium (hexavalent compounds). California Environmental Protection Agency, California.1-97.
- Pechova A, Pavlata L (2007) Chromium as an essential nutrient: a review. Veterinarni Medicina 52(1): 1–18.
- Pizent A, Tariba B, Živković T (2012) Reproductive Toxicity Of Metals In Men. Arh Hig Rada Toksikol 63(1): 35-46.
- Riaz S, Alam SS, Ali G (2006) Effect Of Different Levels Of Chrome Shavings On Hematological Parameters In The Blood Of Quail Chicks. J Ag & Bio Sci 1(1): 23-28.
- Sheiner EK, Sheiner E, Hammel RD, Potashnik G, Carel R (2003) Effect of Occupational Exposures on Male Fertility: Literature Review. Ind Health 41(2):55–62.
- Shrivastava R, Nagar R, Ravishankar GA, Upreti RK, Chaturvedi UC (2007) Effect of pretreatment with chromium picolinate on haematological parameters during dengue virus infection in mice. Indian J Med Res 126(5): 440-446.
- Toghyani M, Shivazad M, Gheisari AA, Zarkesh SH (2006) Performance, Carcass Traits and Hematological Parameters of Heat-Stressed Broiler Chicks in Response to Dietary Levels of Chromium Picolinate. Int J Poult Sci 5(1): 65-69.
- Vinodhini R, Narayanan M (2009) The Impact Of Toxic Heavy Metals On The Hematological Parameters In Common Carp (Cyprinus carpio L.). Iran J Environ Health. Sci Eng 6(1): 23-28.
- Wedeen RP, Qiant L (1991) Chromium-Induced Kidney Disease. Environ Health Perspect 92: 71-74.
- World Health Organization (WHO) 1990. Environmental Health Criteria 61, International Programme on Chemical Safety . Geneva, Switzerland.





