The Role of CD44 Cancer Stem Cell Marker in the Development and Progression of Lymph Node Metastasis in Oral Squamous Cell Carcinoma
Thamer E Alzahrani*
Department of Orthodontic and Dentofacial Orthopedics, Faculty of Dentistry, Taif University, Taif, Saudi Arabia.
*Corresponding Author
Thamer E Alzahrani,
Department of Orthodontic and Dentofacial Orthopedics, Faculty of Dentistry, Taif University, Taif, Saudi Arabia.
Tel: +966569015252
E-mail:tz@tudent.edu.sa
Received: May 21, 2021; Accepted: November 03, 2021; Published: November 09, 2021
Citation: Thamer E Alzahrani. Modified Serial Extraction in Patient with Sever Crowding: A Case Report. Int J Dentistry Oral Sci. 2021;8(10):4923-4926. doi: dx.doi.org/10.19070/2377-8075-21000995
Copyright: Thamer E Alzahrani�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Serial extraction treatment is interceptive treatment to resolve arch length / tooth mass discrepancy. It follows serial extraction of primary teeth to facilitate the eruption of the 1st premolar and then extract it. In our case we present modification for the serial extraction treatmentby extraction of the 2nd premolars instead of the 1rs premolars. We believe that this is good modification to the serial extraction patterns, especially in cases with abnormal eruption sequence.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Interceptive Orthodontic; Serial Extraction; Sever Crowding.
Introduction
Interceptive treatment defined in 1982 by Richardson, he states
that it mean the prompt treatment ofunfavourable features of
a developing occlusion that may makethe difference between
achieving a satisfactory result by simple mechanics later, thus reducing
overall treatment time and providing better stability and
functional and aesthetic results. [1]
The term serial extraction is an example of an interceptive treatment.
It is the correctly timed and planned removal of deciduous
and permanent teeth in mixed dentition cases with sever crowding
to allow the unerupted teeth to guide themselves into better positions
and reduce the long period of fixed appliance therapy. [2]
The classical pattern of serial extraction as the following [3]:
� Stage I: (Extraction of all deciduous lateral incisors). To help in
the alignment of the central incisors.
� Stage II: (Extraction of all deciduous canines after 7�8 months).
For alignment of the lateral incisors
� Stage III: (Extraction of all deciduous first molars). To stimulate
eruption of 1st premolars
� Stage IV: (Extraction of all first premolars after 7�8 months).
This stage provides the space needed for canines and stimulates
their eruption.
The usual eruption pattern is the eruption of the 4s (1st premolar)
a head of the 5s (2nd premolars)[4]. however, in our case
which will be presented below the mandibular 2nd premolars
erupt ahead of the 1st premolars.
Case Report
A twelve-year-old Saudi female patient had a chief complaint of
an irregular teeth came to the orthodontic clinics in Faculty of
dentistry, king Abdelaziz University. Upon extra oral examination
the patient has mesofacial face type , fairly symmetrical face and
competent lips. The profile is slightly convex (Figure 1). Upon
intra-oral examination (figure 2) she had severely inflamed gingiva,
tooth no. 12 and 22 in cross-bite, tooth no. 15 in buccal cross
bite, thin attached gingiva related to tooth no. 41 and Stainlesssteel
crown on tooth no. 46. She has the following permanent
dentition:
- Upper right: 1st molar, 1st and 2nd premolar central and lateral
incisors.
- Upper left: 1st molar, central and lateral incisors.
- Lower left: 1st molar, central and lateral incisors.
- Lower right: 1st molar, 2nd premolar central and lateral incisors.
The crowding had been measured in the dental model (figure 3)
and it showed the following:
� 9 mm crowding in upper arch.
� 8 mm crowding in lower arch.
� Class I molar in the right side.
� Class I molar in the left side.
The panoramic radiographs and cephalometric radiograph are
presented in (figure 4, 5)
A summary for the cephalometric analysis is the following:
- Class I skeletal relationship.
- Hyperdivergent mandible.
- Retroclined upper and lower incisors
The treatment was done as modified serial extraction, (extraction
of the single permanent premolar in each quadrant to allow for
eruption of the canine and resolve the space deficiency) . First, we
extract the primary teeth (53,63,64,65,74) and we also extracted
the permanent tooth number14 then we did band and bond 2*4
appliance to correct the anterior cross bite. (Figure 5) show the
photograph progress at the start of the treatment, then we extract
tooth no. 45(the lower right 2nd premolar erupts ahead of the
1stpremolar) and(Figure 6) shows the radiograph after the extraction
of the lower right premolar.
When the upper left 1st premolar erupted (tooth number 24), we
extracted it, (figure 7) show the progress radiograph. (Figure 8)
show the progress photographs after the extraction of all upper
1st premolar and lower 2ndpremolars, and the panoramic radiograph
is shown in (figure 9).
After the eruption of the lower first premolars and the upper
canines, we bonded them to align them with the arch (figure 10).
(Figure 11,12 ,13) show the final records. While (Figure 14) show
pre and post smile and frontal photographs for the patient.
This case had been treated successfully with a modified serial extraction
plane because the different in the eruption sequence of
the patients in the lower arch.
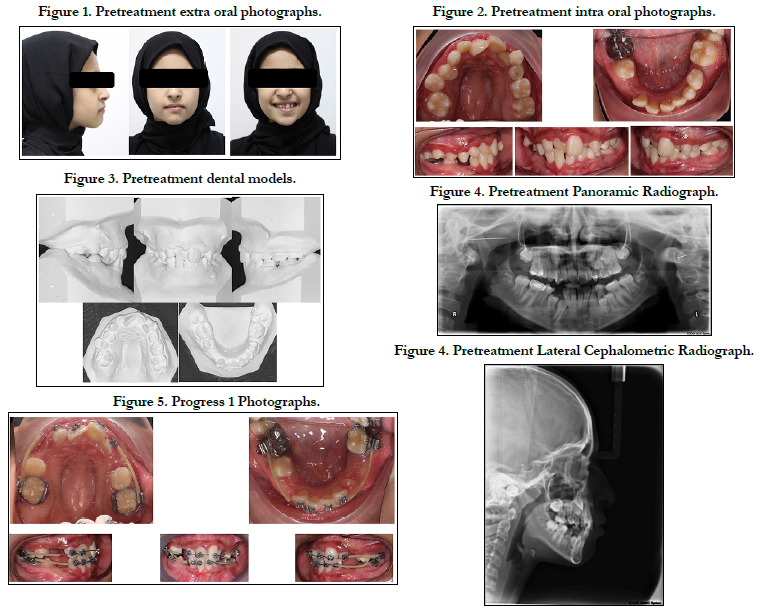
Figure 1-5.
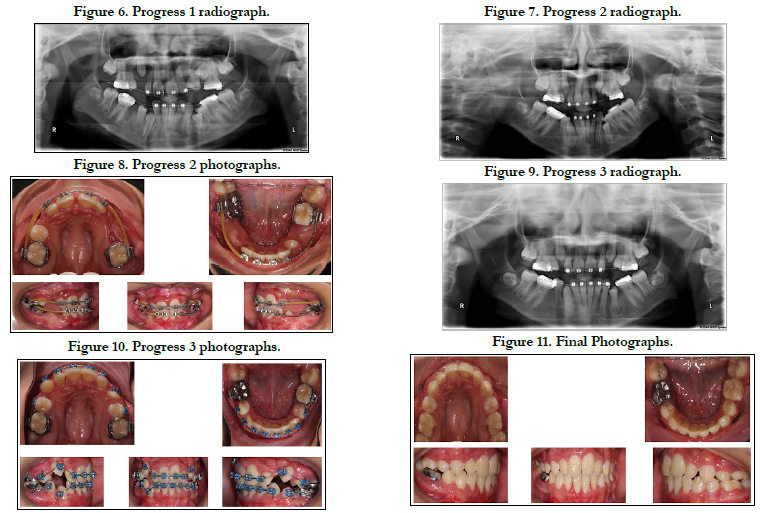
Figure 6-11.
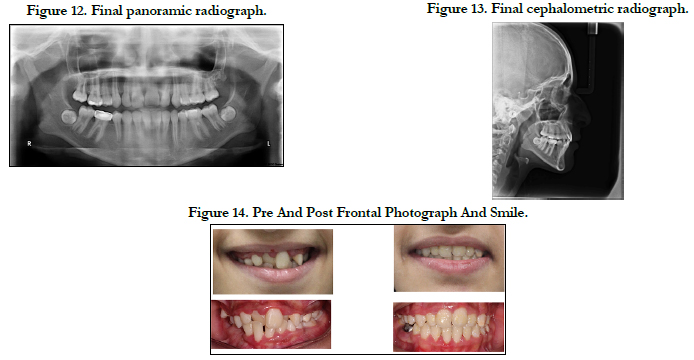
Figure 12-14.
Discussion
The normal eruption time of the succedaneous teeth as the following,
for the upper arch: the central incisors erupt around the
age 7-9 years, lateral incisors 7-9 years, canines 11-12 years, 1st
premolar 10-11 years, 2nd premolar 10-12 years old. So as summary
the sequence as the following: 1,2,4,5,3. While in the lower
arch the eruption the timing of the eruption is the following: central
incisors 6-8 years, lateral incisors 6-8 years, canine 9-10 years,
1st premolar 10-12 years, 2nd premolar 11-12 years old. So as
summary the sequence as the following: 1,2,3,4,5. [4]
There are many benefits in the literature for the early treatment
of sever crowding by serial extraction , it includes the following :
improvement of self-esteem , improve the oral hygiene and better
chewing ability.[5, 6]
Some treatment possibility for the sever crowding in mixed dentition,
is expansion of the arch. However, the stability was poor and
the irregularity index was 6 mm after 7.5 years follow up.[7] In the
other hand, the long term stability with one premolar extraction
was higher and the irregularity index was 4.3 mm [8], 3.5 mm [9]
and 3 mm [10] respectively.
.
Our treatment might be more appropriate to called it (Sequential
Extraction) instead of serial extraction for two reasons. First it
doesn�t follow the same extraction pattern of classical serial extraction.
Second, in serial extraction the aim is to allow the physiological
migration of the teeth into better position, then it followed
by active phase with fixed appliance. However, we started
the fixed appliance treatment in this case early due to the anterior
cross bite.
There are some advantages for second premolars extraction instead
of the first premolars. One of the advantages is the limitation
of the lingual tipping of the mandibular incisors, which will
cause minimum increase of curve of Spee and over bite , further
more maintaining the position of the lower incisors reduce the
flattering of the facial profile [11].
Conclusions
Serial extraction treatment in this patient had been successful in
resolving the arch length/tooth mass discrepancy, resolve the
anterior cross bite and prevented impaction of the canines. The
second premolar extraction can be considered for serial extraction
cases especially in cases with irregular eruption sequence or
expected impaction of the 2nd premolars.
Acknowledgment
I would like to thank Prof. Khalid Zawawi for his continuous support
throughout the treatment.
References
-
[1]. Richardson A. Interceptive orthodontics in general dental practice. Part I-
-Early interceptive treatment. Br Dent J. 1982 Feb;152(3):85�9. Pubmed
PMID: 6949600.
[2]. Mahajan N, Bansal S, Goyal P. Interceptive Orthodontics: A Review. JIDA J Indian Dent Assoc. 2014;8(7).
[3]. Naragond A, Kenganal-Parekh SS, Fields HW. Serial extractions-A review. IOSR J Dent Med Sci. 2012;3:40�473.
[4]. Scott J &symons N. introduction to dental anatomy. 9th editio. 1990. [5]. Yoshihara T, Matsumoto Y, Suzuki J, Sato N, Oguchi H. Effect of serial extraction alone on crowding: relationships between tooth width, arch length, and crowding. Am J Orthod Dentofac Orthop Off Publ Am Assoc Orthod its Const Soc Am Board Orthod. 1999 Dec;116(6):691�6. Pubmed PMID:10587605.
[6]. Dale JG. Serial extraction ... nobody does that anymore! Am J Orthod Dentofac Orthop Off Publ Am Assoc Orthod its Const Soc Am Board Orthod. 2000 May;117(5):564�6. Pubmed PMID:10799116.
[7]. Little RM, Riedel RA, Stein A. Mandibular arch length increase during the mixed dentition: postretention evaluation of stability and relapse. Am J Orthod Dentofac Orthop Off Publ Am Assoc Orthod its Const Soc Am Board Orthod. 1990 May;97(5):393�404. Pubmed PMID:2333853.
[8]. Little RM, Riedel RA, Engst ED. Serial extraction of first premolars--postretention evaluation of stability and relapse. Angle Orthod. 1990;60(4):255� 62. Pubmed PMID:2256562.
[9]. McReynolds DC, Little RM. Mandibular second premolar extraction-- postretention evaluation of stability and relapse. Angle Orthod. 1991;61(2):133�44. Pubmed PMID:2064071.
[10]. Haruki T, Little RM. Early versus late treatment of crowded first premolar extraction cases: postretention evaluation of stability and relapse. Angle Orthod. 1998 Feb;68(1):61�8. Pubmed PMID:9503136.
[11]. Joondeph DR, Riedel RA. Second premolar serial extraction. Am J Orthod. 1976;69(2):169�84. Pubmed PMID:1061507.





