Non-Operative Management of Knee Osteoarthritis Disability
Marks R1,2*
1 Department of Health and Behavior Studies, Program in Health Education, Columbia University, Teachers College, USA.
2 School of Health and Behavioral Sciences, Department of Health, Physical Education & Gerontological Studies and Services, City University of New
York, York College, New York, USA.
*Corresponding Author
Dr. Ray Marks,
Department of Health and Behavior Studies,
Columbia University,Teachers College, Box 114,
525W 120th Street, New York, NY 10027,
USA.
Tel: 1-212-678-3445
Fax: 1-212-678-8259
E-mail: rm226@columbia.edu
Article Type : Review Article
Received: October 19, 2015; Accepted: November 16, 2015; Published: November 18, 2015.
Citation: Marks R (2015) Non-Operative Management of Knee Osteoarthritis Disability. Int J Chronic Dis Ther 1(2) 9-15. doi: dx.doi.org/10.19070/2572-7613-150003
Copyright: Marks R© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Knee osteoarthritis, a highly common, disabling joint disease affecting a large number of older adults is presently incurable, and not always amenable to surgery or pharmacologic interventions.
Purpose: The purpose of the present review was to describe the nature of osteoarthritis and examine the utility of some non-pharmacological and non-operative treatment strategies that have been advocated for alleviating the pain and disability of knee osteoarthritis in later life.
Methods: A review of the English language data base was conducted to identify relevant literature published on this topic over the last 35 years. Key words included osteoarthritis, knee, and management.
Results: As with other forms of osteoarthritis, osteoarthritis of the knee produces considerable disability and impedes the attainment of a high life quality for many older adults. Alone or in combination, several non-operative and non-pharmacologic approaches may however, influence the disease process quite favourably, and promote more favourable functional outcomes than standard care practices commonly yield.
Conclusions: The application of one or more carefully designed conservative interventions is likely to reduce the functional disability and pain experienced by older people with knee osteoarthritis, regardless of whether surgical and or pharmacologic strategies are indicated.
2.Introduction
3.Osteoarthritis
4.Knee Osteoarthritis
5.Management Strategies
6.Treatment Approaches
6.1.Education
6.2.Joint protection strategies
6.3.Physical modalities
6.4.Exercises
7.Conclusion
8.References
Keywords
Aging; Disability; Management; Knee Joint Osteoarthritis; Outcomes.
Introduction
Osteoarthritis, the most common rheumatic disease, is a chronic non-fatal condition with significant individual, social and economic ramifications [1-3]. Principally due to localized disruptions in the articular cartilage tissue lining all freely moving joints of the body, osteoarthritis often causes varying degrees of painful mechanical dysfunction [2] that can severely impair an individual's ability to function physically without compromise [3]. Unfortunately, while useful in restoring function and ameliorating pain in severe cases of the disease, not all cases of osteoarthritis may be amenable to artificial joint-replacement surgery, especially if multiple joint sites are affected. Reducing osteoarthritic pain by means of analgesic medication and non-steroidal anti-inflammatory drugs, also frequently proves ineffective or harmful [2].
In seeking to assist people with osteoarthritis, who are frequently 60 years or older, to meet the challenges of daily life as optimally as possible, a wide array of adjunctive methods other than medications, or surgery that might reduce the pain and disability associated with osteoarthritis, and are cost effective, have consequently been advocated. Yet, while somewhat effective in selected cases, patients may report not being sufficiently educated about the disease and its treatment options, and prognosis [4]. Many too, may not employ or engage in any non-pharmacologic strategy even though these are recommended before surgical treatment options are considered [5]. With few definitive studies that have examined the application of personalized comprehensive evaluations followed by carefully construed and selected strategies on the disease outcome, both clinicians as well as patients may not feel confident in generalizing the idea of conservative treatments for treating osteoarthritis. Patients who are aware, may also vary widely even if they have the same diagnosis, thus careful tailoring of recommendations is indicated. Patients especially, may not be sufficiently enthused towards applying the principles of disease self-management [6] if their providers do not mention the importance of this approach.
Since there is increasing evidence that the rates of disability produced by osteoarthritis are not inevitable, but that lifestyles and behaviours have powerful influences as well, the objective of this brief was to review the chief characteristics of osteoarthritic joint disease, especially components of the disease that might be positively affected by one or more non-pharmacologic strategies, and to consider how knee osteoarthritis, the most common form of the disease, might be managed effectively by conservative nonpharmacologic approaches given that these are cost-effective and often successful [7]. Although directed towards a conservative prescription for the management of knee osteoarthritis, the most important causes of pain and physical disability in the community [8], the therapeutic rationale outlined should be applicable to other joint sites commonly affected by osteoarthritis.
To this end the PubMed, Scopus, and Web of Science data bases between 1990-2015 were examined using key words, osteoarthritis, knee joint, self-management, treatment. Although some work has been implemented to systematically review the research in this realm, most studies are somewhat flawed, focus on diverse topics, samples, and joint status, precluding any useful quantitative synthesis at the present time. The data extracted were hence categorized according to the disease itself, and those research data that could be used to address the perspective of self-management as a component of conservative and surgical interventions, rather than clinic based therapies.
Osteoarthritis
Osteoarthritis, often neglected as a serious health condition, produces an untold burden and costly outcome for adults of all ages, especially the elderly. Although the pathology of osteoarthritis, which entails the presence of focal or complete lesions of the articular cartilage lining of one or more joints, as well as various degrees of bone remodelling and exposure of underlying bone, is well established, and accumulated knowledge shows some of this disability is amenable to prevention or intervention, very few preventative efforts to counter these changes exist. One reason for this may be a failure of clinicians and others to carefully scrutinize the available current research, and to rely on historical myths that osteoarthritis is inevitable and irreversible, and that radiological joint changes equate to clinical osteoarthritis (See Box 1). Hence, both persons with the condition as well as their providers may simply believe the disease is inevitable, and that thoughts of reversing this condition are ‘heresy’. As a result, in addition to neglecting the idea that chondrocytes can respond favourably to optimal intracellular signals, other pathological features of the disease process such as various degrees of joint capsular and synovial membrane thickening, joint inflammation, ligament and tendon damage, and muscle pathology and atrophy, which may respond to targeted treatments, may go untreated and as a result may hasten chondrocyte cell death and ensuing joint destruction processes [9].
Box 1. Myths Concerning Osteoarthritis
- Osteoarthritis reflects the passive erosion of cartilage that is irreversible
- Radiological changes are equated with clinical osteoarthritis
- Osteoarthritis is inevitable
- Osteoarthritis is an old person’s disease
- Articular cartilage has no reparative properties
- Not much can be done to impact the disease
- Treatments are of little help [98]
This is unfortunate because as a result of the above mentioned pathological changes and others, the hallmark symptomatic feature of osteoarthritic destruction, namely pain, may be unremitting and accompanied by extended periods of joint stiffness after rest, which may last longer than 30 minutes; the possible onset of diminished or excessive joint range of motion, joint tenderness, joint crepitus or ‘locking’ on motion, variable degrees of joint inflammation, and joint swelling [8]. There may also be a decline in joint stability and overall function, plus evidence of irreversible joint deformity and malalignment. Anxiety, depression, and impaired psychosocial functioning, along with a decreased selfimage are also frequent undesirable outcomes of osteoarthritis, as are impairments of general health, and vitality [10]. Consequently, although not usually fatal, the signs and symptoms of osteoarthritis may severely reduce the ability of an individual to carry out his or her normal activities of daily living without undue stress [11], and may limit work capacity and wage earnings quite considerably [12]. In the geriatric years, the disease may seriously compromise life quality [10] and the ability to live independently and carry out self-care activities [8].
On the other hand, results of some in vitro studies provide tentative evidence that the abnormal biochemically and biomechanically mediated cell-matrix interactions of osteoarthritic cartilage that usually result in an overall loss of its compressive stiffness and elasticity [13], may be part of an attempted reparative process [14]. In particular, because mechanical stimuli are essential for the growth and maintenance of cartilage and aberrant mechanical loading can lead to cartilage damage, it appears that careful mechanical manipulation of the cell micro-environment may arguably help to foster tissue reconstitution and reduce cartilage matrix damage attributable to the release of degradative enzymes by damaged cartilage cells [15]. This is supported by numerous loading studies ranging from immobilization to excessive weightbearing [16] and others that imply that excessive repetitive impacts or preventable mechanical insults might potentiate cartilage damage or render the bone beneath this tissue noncompliant [16].
In sum, osteoarthritis may not be inevitable, in all cases, and even when present may be amenable to amelioration if careful evaluations followed by carefully construed and timely treatment strategies are forthcoming.
Knee Osteoarthritis
The knee, a commonly involved joint affected by osteoarthritis [8], is a frequent source of functional disability and pain [17], especially in the elderly [18] and women who may have decreased survival rates [19]. Linked strongly with bone marrow lesions [20], and obesity in bilateral cases and knee injury in unilateral cases [21], the individual and collective socio-economic impact attributable to knee osteoarthritis is considerable [22].
As with osteoarthritis in general, knee osteoarthritis is commonly accompanied by one or more of the following disabling signs and symptoms: knee pain on motion, decreased knee range of motion, knee muscle weakness, knee joint swelling and inflammation, instability and deformity [23-27]. Also frequently evident are gait abnormalities [28], a diminished aerobic capacity [29], and limitations in function with respect to rising from a chair, stair climbing and squatting [30].
Contributing to these clinical problems may be several physical factors including abnormalities in the motor unit physiology of one or more of the knee extensor muscles. There may also be extensive knee extensor muscle pathology, a very high rate of knee extensor muscle protein degradation and related problems of impaired knee proprioception, knee muscle inhibition due to swelling, and postural instability [32-37] plus loss of functional independence [38].
Fortunately, there is evidence that most individuals with knee osteoarthritis can be treated reasonably successfully by sustained adherence to a well-designed conservative management program, including patient education, nutrition counselling, exercise instruction, and home and work modifications [7], especially if these interventions are implemented in the early phases of the disease [39]. Moreover, the degree of disability arising from knee osteoarthritis may not be inevitable if carefully construed efforts to minimize future joint insults, increase surrounding muscle strength and power, and reduce pain and inflammation are forthcoming.
Management Strategies
In light of the possibility that osteoarthritic cartilage repair processes may exist [40], non-pharmacological and non-operative interventions that carefully consider all possible pathogenic mechanisms that contribute to the disease, may merit investigation [41]. They may also be effective for reducing functional limitations and disability, the health factor of most concern to patients [42].
In particular, given that subnormal joint loading mechanisms strongly influences the osteoarthritis disease process [43], eliminating the most detrimental forces falling on the joint surface, as well as improving the ability of the surrounding tissues to absorb, distribute and respond to mechanical forces more physiologically, is likely to prove especially helpful, irrespective of causative mechanism [44]. Encouraging movements to optimize a healthy joint range of motion and facilitate joint nutrition might also be expected to similarly promote some degree of cartilage repair or reversal of cartilage catabolism, while relieving pain and enhancing quality of life, particularly during the early stages of the disease process [45].
Interventions in this respect might include a variety of joint protection and energy conservation strategies, exercise regimens, and the application of a variety of physical modalities that relieve pain and enhance muscle function and intermittent joint compression. Moreover, being active and productive, and keeping a healthy weight is likely to prove more useful than not.
To ascertain what might produce the most optimal result for an individual, the clinician can help by undertaking a thorough history and physical examination before ascertaining whether the intervention aim is to achieve: 1) a reduction in knee joint pain, knee muscle spasm and/or swelling, 2) an increase in knee mobility, stability, strength, endurance, proprioception, balance control and/or gait efficiency, and/or 3) optimal aerobic fitness or weight control. They can also conduct a mental health screening test to examine whether depression, anxiety, or stress are likely to be factors requiring additional intervention attention. Ascertaining the magnitude of the osteoarthritic condition, and the client’s general health status will also be helpful, along with other measures depicted in Box 2.
Box 2. Assessment Profile
Demographic information
- Age
- Gender
- Educational level
- Weight
- Height
- Comorbid health conditions-Number and type
- Joints affected
- Duration condition
- Medications used-number and type
- Mental health status-
- Other treatments- past and present
- Occupation
- Quality of life
Recommended assessment components
- Balance, instability, buckling
- Body mass impedance test to assess body mass category
- Depression and anxiety
- Energy cost of walking
- Exercise self-efficacy
- Gait kinematics, and kinetics
- Inflammation
- Knee function
- Loading frequency
- Malalignment, deformity, contractures
- Muscle strength, endurance
- Osteoarthritis knowledge
- Pain assessment-VAS, McGill Questionnaire
- Range of motion
- Self-efficacy expectation questionnaire
- Self-paced walking, sit to stand and stair climbing tests
Other
Treatment Approaches
Regardless of the aim of any therapeutic strategy, because both helplessness and a lack of education appear to be highly important, potentially treatable factors in determining the extent of knee osteoarthritis disability [46], patient education is highly recommended [47]. In addition to explaining the general principles discussed previously, the educational component for knee osteoarthritis should address the need to balance rest with activity.
To effectively meet the goals and objectives of educating the patient about his or her condition, the selected approach developed in conjunction with input from the patient should help to: (a) promote adoption of any desirable or required novel behavior(s), (b) facilitate adherence and maintenance of the behavior(s); (c) prevent relapse of unhealthy behavior(s) [48]. Desirable educational interventions likely to be most effective are those that employ a skilled empathetic interventionist with a positive outlook, and the use of behavioral contracting, generalization training, and commitment strategies. Written exercise and/or nutrition instructions and others with diagrams understandable by both the patient and their significant others are especially important. Finally, to mitigate the impact of depression due to the disease chronicity, helping to build the patient’s confidence by enacting small achievable steps and appropriate feedback as outlined by self-efficacy theory [49], plus emotional support for both patients and caregivers has been recommended in educational programming [50].
Although there is little empirical evidence to support the implementation of joint protection and energy conservation strategies for knee osteoarthritis [51], appliances such as canes [51] and unloader braces, and neoprene sleeves or splints may help to protect the joint from excessive stresses [52]. Such devices are particularly valuable in the presence of muscle weakness, malalignment and instability of the lower leg. Likewise, orthotic devices that facilitate or improve function by fostering the favorable application of biomechanical forces and hence the magnitude of joint stresses falling on the medial or lateral compartments, may be of benefit [53], as may the use of well-cushioned shoes [51]. Other modalities that may afford joint protection secondarily include interventions such as patellar taping [54] and insoles [55]. For overweight individuals, weight loss to reduce the impact loads at the knee and poor knee muscle function that can cause further joint damage may help slow the progression of knee osteoarthritis [56].
In addition to the previously mentioned strategies, educating the patient about the adverse impact of engaging in prolonged periods of standing, kneeling and squatting, walking at rapid speeds and engaging in sports or work activities that increase stress on the joint or involve jarring or unexpected movements, as well as fatiguing activities is recommended [53]. Avoiding the use of stairs and low chairs, showering instead of bathing, or using aids to minimize joint forces generated by these activities is also desirable. To minimize joint stress and conserve energy, a well-planned well-organized work space that facilitates use of efficient body mechanics and includes periods of rest coupled with periods of modest activity during the day is also advocated. However, completely unweighting the joint for example for exercise purposes may not prove effective in decreasing pain in the long term [57].
Because of the strong possibility that muscle may be implicated in some aspects of the osteoarthritic disease process at the knee, physical interventions other than exercise that improve muscle function may prove beneficial. These include modalities that can be applied at home such as ice [58], heat [59], and electromyographic biofeedback-controlled exercise training that uses an audio or visual signal to provide feedback on the prevailing versus the desired muscle functional outcome, [60] and can reduce muscle spasm and pain. In addition, transcutaneous electrical stimulation treatments, that uses an electrical current and small electrodes attached to a portable transmitter to override pain signals in around the affected joint[s] can help to improve functional status, and for those who incur too much discomfort with active exercises electrical muscle stimulation may provide an appropriate alternative to this form of activity [61].
Knee joint proprioception, muscle reflex activation, strength, and joint range of motion and stability, all compromised in knee osteoarthritis, may all be improved by carefully designed therapeutic exercises, such as strength training, range of motion exercises, stretching, and postural exercises [62, 63]. In turn improved muscle strength may also foster bone mineralization, cartilage repair [62], endorphin production [62], and central factors known to affect peripheral pain, such as anxiety [62, 64]. Other physiological benefits of therapeutic strengthening exercise for the osteoarthritic knee include increments in the tensile strength of the surrounding joint capsular, tendon and ligamentous tissues [17], improved post-exercise joint blood flow and cartilage nutrition [65], venous and lymphatic return [66] and synovial blood flow [67].
However, although most studies report a positive effect on pain or disability regardless of exercise protocol [68], recommendations for exercise may not be forthcoming, and thus patients may not find their condition is improving [69]. Others may not consider the importance of acknowledging osteoarthritic complications such as joint effusion, muscle pathology, instability, and fatigue [70] in detrimentally influencing the outcomes of any exercise prescription [71]. Many patients too may have high blood pressure, which may not be well controlled, and caution is hence advised in prescribing exercises to these individuals, without careful deliberation and instruction. Similarly, care must be taken to caution those with knee hypermobility or instability about the consequences of overstretching, and incurring fatigue.
To be effective, exercise prescriptions should also take into account the individual's personal needs, preferences and interests, as well as their psychosocial status, and perceived self-efficacy for undertaking exercises and for achieving successful outcomes as discussed by Kovar et al. [72]. Cross-training or exercising at various muscle lengths, speeds and intensity, may also allow exercises carried out to have both specific positive, as well as generalized benefits [67, 73]. Because compliance with exercise has been found to improve if exercise is perceived as recreational, the use of a warm pool or group exercises with musical accompaniment has been recommended [74].
In short, unlike medications which do not reverse the disease process [76], a significant proportion of cases with knee osteoarthritis studied to date are likely to show adequate symptom relief in response to one or more conservative therapeutic approaches such as weight loss, exercise, the use of physical modalities [77], efforts to optimize joint biomechanics [78], and self-efficacy [79]. In contrast, a lower life quality, and more rapid extensive pathology and disability is likely to ensue by failure to follow a long-term regime of joint protection, exercise, and weight control, regardless of whether or not pharmacolic and/or surgical strategies are indicateds.
Conclusion
Osteoarthritis, a common painful disabling disease, frequently affecting the knee joint, often thought to be untreatable, can be favourably impacted by a variety of conservative management approaches applied alone, or in combination, including, but not limited to, patient education, weight reduction, the appropriate application of assistive devices and orthotics, exercises to maximize muscle strength and endurance, joint range of motion and aerobic capacity, among others. That is, carefully tailored and personalized uni-or multicomponent approaches recommended in light of the extent of prevailing joint destruction, and the patient’s age, health status, beliefs, fears, anxieties, and general capabilities for self-management can potentially yield quite favorable rather than unfavourable disease outcomes [75, 98].
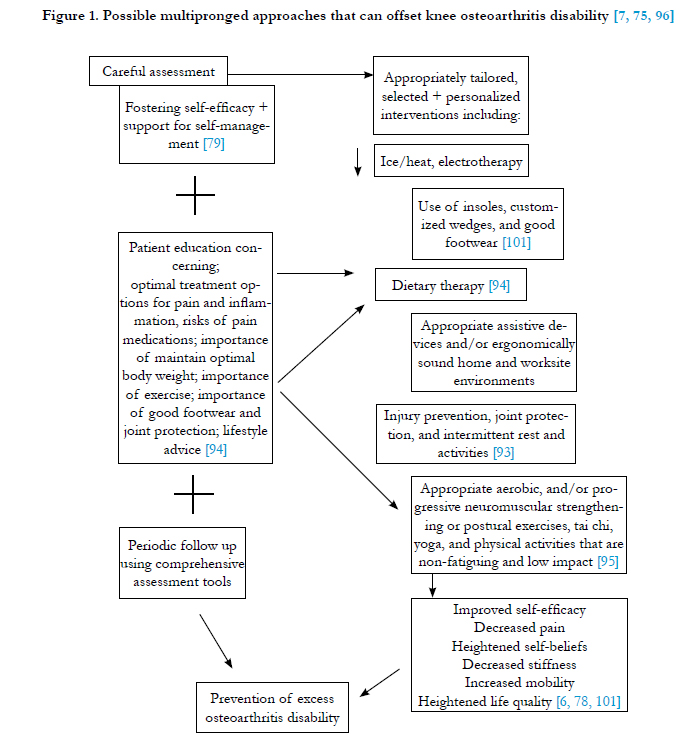
However, because pain relief that leads to excessive joint use could have adverse effects on damaged cartilage [80], a structure very sensitive to mechanical signals [81], enabling the patient’s understanding of all potential contributing factors to the prevailing structural damage and dysfunction, such as loading magnitude and frequency [81], is desirable in efforts to reduce their pain and prevent excess disability, while promoting independence, as well as life quality [82, 83] as outlined in Figure 1.
In particular, educating the patient to assert control over their disease, and that excessive fatigue can have a highly negative impact on the patient’s life [84] is as important as helping patients to pursue realistic treatment goals and expectations. In addition, efforts to avoid injury and/or excessive loading of an osteoarthritic knee, especially if a sensory deficit prevails [85] should be stressed. Making patients aware that their own self-management practices may not only benefit joint regeneration processes [86], but may minimize the degree of any associated inflammation [87-89], while improving their life quality, is also of great import in efforts to foster adoption and adherence of self-management recommendations as outlined by Smith et al. [6]. Finally, dispelling the myth that osteoarthritis is inevitable, and revealing the promising results of many current non-pharmacologic intervention studies when viewed independently [e.g. [7, 76]], along with their low risks of side-effects or long term health concerns, might provide patients as well as providers with a strong rationale for pursuing and adhering to such programs.
In this regard, given the failure of prevailing pharmacologic and surgical interventions to prevent disability in all cases, future research to investigate the long-term benefits of the various conservative intervention approaches that have shown promise to date or have been discussed in the related literature should be explored further [eg [90-97]]. As well, whether any of these recommended approaches can assist in efforts to improve cartilage regeneration efforts [86] and can minimize inflammation that can worsen structural damage [87], while improving the mechanical environment of the knee joint [57], also awaits further research.
However, as discussed by Roos and Arden [90] it is the present author’s view that to correct or attenuate osteoarthritic symptomology, efforts to examine exactly what is most appropriate as well as acceptable for the individual patient, followed by well construed education and provision of resources and prescriptive advice will markedly optimize adherence to-and persistence withthese regimes. It is also the author’s view that even if such an approach does not prevent the progression of the disease or reverse it, health status as a whole is likely to be more positively impacted than not by employing these aforementioned non pharmacologic self-management directives as outlined by Haung et al. [91], Anwere [92], Harris and Crawford [93].
As outlined by Walker [97], for many older people with knee osteoarthritis, the ability to engage or not engage in meaningful social actions and functional activities promises to be ably facilitated by the strategies discussed in here, including a holistic assessment and tailored interventions as outlined Box 2 and Figure 1. Other non-pharmacoligic approaches not discussed here that depend on more passive strategies or group activities among others, should also not be overlooked.
References
- Shi D, Dai J, Xu Z, Chen D, Jiang Q (2015) Update on basic and clinicalaspects of osteoarthritis. Ann Transl Med 3(10): 142.
- Simon LS (1999) Osteoarthritis: a review. Clinical Cornerstone 2(2): 26-37.
- Jordan JM. (2015) An ongoing assessment of osteoarthritis in African Americans and Caucasians in North Carolina: The Johnston County Osteoarthritis Project. Trans Am Clin Climatol Assoc 126: 77-86.
- Haskins R, Henderson J, Bogduk N. (2014) Health professional consultation and use of conservative management strategies in patients with knee or hip osteoarthritis awaiting orthopaedic consultation. Austral J Primary Hlth 20: 305-310.
- Van Manen MD, Nace J, Mont MA. (2012) Management of primary knee osteoarthritis and indications for total knee arthroplasty for general practitioners. J Am Osteopath Assoc 112(11): 709-715.
- Smith T, Purdy R, Lister S, Salter C, Fleetcroft R, et al. (2014) Attitudes of people with osteoarthritis towards their conservative management: a systematic review and meta-ethnography. Rheumatol Int 34(3): 299-313.
- Snijders GF, den Broeder AA, van Riel PL, Straten VH, de Man FH, et al. (2011) Evidence-based tailored conservative treatment of knee and hip osteoarthritis: between knowing and doing. Scandinav J Rheumatol 40(3):225-231.
- Ling SM, Bathon JM (1998) Osteoarthritis in older adults. J Am Geriatr Soc 46(2): 216-225.
- Dieppe P (1990) Some recent clinical approaches to osteoarthritis research. Semin Arthritis Rheum 20(3): 2-11.20: 2-11.
- Briggs A, Scott E, Steele K (1999) Impact of osteoarthritis and analgesic treatment on quality of life of an elderly population. Ann Pharmacother 33(11): 1154-1159.
- Yelin E, Lubeck D, Holman H, Epstein W (1987) The impact of rheumatoid arthritis and osteoarthritis: the activities of patients with rheumatoid arthritis and osteoarthritis compared to controls. J Rheumatol 14(4): 710-716.
- Buckwalter JA, Martin J, Mankin HJ. (2000) Synovial joint degeneration and the syndrome of osteoarthritis. Instructional Course Lect 49: 481-489.
- Kuettner KE (1992) Biochemistry of articular cartilage in health and disease. Clin Biochem 25(3): 155-163.
- Brocklehurst R, Bayliss MT, Maroudas A, Coysh HL, Freeman MA, et al. (1984) The composition of normal and osteoarthritic articular cartilage from human knee joints. With special reference to unicompartmental replacement and osteotomy of the knee. J Bone Joint Surg Am 66(1): 95-106.
- Marks R (1991) Effect of altered functional demand on the structural and functional properties of articular cartilage. New Zealand J Physiother 19: 31-34.
- Marks R (1992) Physical modalities and articular cartilage repair. New Zealand J Physiother 20: 17-20.
- Marks R (2015) Muscle and muscle mechanisms as possible factors leading to osteoarthritis. SM J Orthop 1(2). http://smjournals.com/index.php/orthopedics/article/view/153
- Felson DT, Naimark A, Anderson J, Kazis L, Castelli W, et al. (1987) The prevalence of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum 30(8): 914-918.
- Lawrence RC, Everett DF, Cornoni-Huntley J (1987) Excess mortality and decreased survival in females with osteoarthritis (OA) of the knee. ARA 51st annual meeting. Washington DC.
- Wluka AE, Teichtahl AJ, Maulana R, Liu BM, Wang Y, et al. (2015) Bone marrow lesions can be subtyped into groups with different clinical outcomes using two magnetic resonance imaging (MRI) sequences. Arthritis Res Ther 17: 270.
- Davis MA, Ettinger WH, Neuhas JM, Cho SA, Hauck WW (1989) The association of knee injury and obesity with unilateral and bilateral osteoarthritis of the knee. Am J Epidemiol 130(2): 278-288.
- Hadler NM (1985) Osteoarthritis as a public health problem. Clin Rheum Dis 11(2): 175-185.
- Madsen OR, Brot C, Petersen MM, Sørensen OH (1987) Body composition and muscle strength in women scheduled for a knee or hip replacement. A comparative study of two groups of osteoarthritic women. Clin Rheumatol 16(1): 39-44.
- Nordesjo LO, Nordgren B, Wigren A, Kolstad K (1983) Isometric strength and endurance in patients with severe rheumatoid or osteoarthritis in the knee joint. Scandinav J Rheumatol 12(2): 152-156.
- Slemenda C, Brandt KD, Heilman DK, Mazzuca S, Braunstein EM, et al. (1997) Quadriceps weakness and osteoarthritis of the knee. Ann Int Med 127(2): 97-104.
- Tan J, Balci N, Sepici V, Gener FA (1995) Isokinetic and isometric strength in osteoarthrosis of the knee. A comparative study with healthy women. Am J Phys Med Rehabil 74(5): 364-369.
- Staudte HW, Brussatis F (1977) Selective changes in size and distribution of fibre types in vastus muscle from cases of different knee joint affections.Z Rheumatol 36(5-6): 143-160.
- Waters RL, Perry J, Conaty P, Lunsford B, O'Meara P (1987) The energy cost of walking with arthritis of the hip and knee. Clin Orthop Relat Res (214): 278-284.
- Minor MA, Hewett JE, Webel RR, Anderson SK, Kay DR (1989) Efficacy of physical conditioning exercise in patients with rheumatoid arthritis and osteoarthritis. Arthritis Rheum 32(11): 1396-1405.
- Whitchelo T, McClelland JA, Webster KE (2014) Factors associated with stair climbing ability in patients with knee osteoarthritis and knee arthroplasty: a systematic review. Disabil Rehabil 36(13): 1051-1060.
- Brucini M, Duranti R, Galleti R, Pantaleo T, Zucchi PL (1981) Pain thresholds and electromyographic features of periarticular muscles in patients with osteoarthritis of the knee. Pain 10(1): 57-66.
- Marks R, Kumar S, Percy J, Semple J (1995) Force-time measurements of the quadriceps femoris muscles of healthy women and women with osteoarthrosis of the knee. Eur J Phys Med Rehabil 5: 88-92.
- Marks R, Percy J, Semple J, Kumar S (1994) Comparison between the surface electromyogram of the quadriceps surrounding the knees of healthy women and the knees of women with osteoarthrosis. Clin Exp Rheumatol 12(1): 11-15.
- Gibson JN, Morrison WL, Scrimgeour CM, Smith K, Stoward PJ, et al. (1989) Effects of therapeutic percutaneous electrical stimulation of atrophic human quadriceps on muscle composition, protein synthesis and contractile properties. Eur J Clin Invest 19(2): 206-212.
- Røsland T, Gregersen LS, Eskehave TN, Kersting UG, Arendt-Nielsen L (2015) Pain sensitization and degenerative changes are associated with aberrant plantar loading in patients with painful knee osteoarthritis. Scand J Rheumatol 44(1): 61-69.
- Alnahdi AH, Zeni JA, Snyder-Mackler L (2012) Muscle impairments in patients with knee osteoarthritis. Sports Health 4(4): 284-292.
- Khalaj N, Abu Osman NA, Mokhtar AH, Mehdikhani M, Wan Abas WA (2014) Balance and risk of fall in individuals with bilateral mild and moderate knee osteoarthritis. PLoS One 9(3): e92270.
- Alkjaer T, Raffalt PC, Dalsgaard H, Simonsen EB, Petersen NC, et al. (2015) Gait variability and motor control in people with knee osteoarthritis.Gait Posture pii: S0966-6362(15)00792-4.
- Cho H, Pinkhassik E, David V, Stuart JM, Hasty KA (2015) Detection of early cartilage damage using targeted nanosomes in a post-traumatic osteoarthritis mouse model. Nanomedicine 11(4): 939-946.
- Perry GH, Smith MJ, Whiteside CG (1972) Spontaneous recovery of the joint space in degenerative hip disease. Ann Rheumatic Dis 31(6): 440-448.
- Tiku ML, Sabaawy HE (2015) Cartilage regeneration for treatment of osteoarthritis: a paradigm for nonsurgical intervention. Ther Adv Musculoskelet Dis 7(3): 76-87.
- Creamer P, Lethbridge-Cejku M, Hochberg MC (1999) Determinants of pain severity in knee osteoarthritis: effect of demographic and psychosocial variables using 3 pain measures. J Rheumatol 26(8): 1785-1792.
- Takeda H, Nakagawa T, Nakamura K, Engebretsen L (2011) Prevention and management of knee osteoarthritis and knee cartilage injury in sports.Br J Sports Med 45(4): 304-309.
- Lane NE, Thompson JM (1997) Management of osteoarthritis in the primary- care setting: An evidence-based approach to treatment. Am J Med103(6A): 25S-30S.
- Blalock D, Miller A, Tilley M, Wang J (2015) Joint instability and osteoarthritis. Clin Med Insights Arthritis Musculoskelet Disord 8: 15-23.
- Cleveland RJ, Luong ML, Knight JB, Schoster B, Renner JB, et al. (2013) Independent associations of socioeconomic factors with disability and pain in adults with knee osteoarthritis. BMC Musculoskelet Disord 14(1): 297.
- Fibel KH, Hillstrom HJ, Halpern BC (2015) State-of-the-Art management of knee osteoarthritis. World J Clin Cases 3(2): 89-101.
- Allegrante JP, Kovar PA, MacKenzie CR, Peterson MG, Gutin B (1993) A walking education program for patients with osteoarthritis of the knee: theory and intervention strategies. Health Educ Q 20(1): 63-81.
- Yip YB, Sit JW, Fung KK, Wong DY, Chong SY, et al. (2007) Effects of a self-management arthritis programme with an added exercise component for osteoarthritic knee: randomized controlled trial. J Adv Nurs 59(1): 20-28.
- Bagge E, Brooks P (1995) Osteoarthritis in older patients. Optimum treatment. Drugs and Aging 7: 176-183.
- Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, et al. (2013) EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis 72(7): 1125-1135.
- Chuang SH, Huang MH, Chen TW, Weng MC, Liu CW, et al. (2007) Effect of knee sleeve on static and dynamic balance in patients with knee osteoarthritis. Kaohsiung J Med Sci 23(8): 405-411.
- Fu HC, Lie CW, Ng TP, Chen KW, Tse CY, et al. (2015) Prospective study on the effects of orthotic treatment for medial knee osteoarthritis in Chinese patients: clinical outcome and gait analysis. Hong Kong Med J 21(2):98- 106.
- Cho HY, Kim EH, Kim J, Yoon YW (2015) Kinesio taping improves pain, range of motion, and proprioception in older patients with knee osteoarthritis: a randomized controlled trial. Am J Phys Med Rehabil 94(3): 192-200.
- Stemberger R, Kerschan-Schindl K (2013) Osteoarthritis: physical medicine and rehabilitation--nonpharmacological management. Wien MedWochenschr 163(9-10): 228-235.
- Teichtahl AJ, Wluka AE, Wang Y, Wijethilake PN, Strauss BJ, et al. (2015) Vastus medialis fat infiltration – a modifiable determinant of knee cartilage loss. Osteoarthritis Cartilage pii: S1063-4584(15)01225-X.
- Farrokhi S, Voycheck CA, Tashman S, Fitzgerald GK (2013) A biomechanical perspective on physical therapy management of knee osteoarthritis. J Orthop Sports Phys Ther 43(9): 600-619.
- Yurtkuran M, Kocagil T (1999) TENS, electroacupuncture and ice massage: comparison of treatment for osteoarthritis of the knee. Am J Acupunct 27(3-4): 133-140.
- Brosseau L, Yonge KA, Robinson V, Marchand S, Judd M, et al. (2003) Thermotherapy for treatment of osteoarthritis. Cochrane Database Syst Rev (4):CD004522.
- Choi YL, Kim BK, Hwang YP, Moon OK, Choi WS (2015) Effects of isometric exercise using biofeedback on maximum voluntary isometric contraction, pain, and muscle thickness in patients with knee osteoarthritis. J Phys Ther Sci 27(1): 149-153.
- Vance CG, Rakel BA, Blodgett NP, DeSantana JM, Amendola A, et al. (2012) Effects of transcutaneous electrical nerve stimulation on pain, pain sensitivity, and function in people with knee osteoarthritis: a randomized controlled trial. Phys Ther 92(7): 898-910.
- Marks R (1992) Peripheral articular mechanisms in pain production in osteoarthritis. Aust J Physiother 38(4): 289-298.
- Nejati P, Farzinmehr A, Moradi-Lakeh M (2015) The effect of exercise therapy on knee osteoarthritis: a randomized clinical trial. Med J Islam Repub Iran 29:186.
- Thomas KS, Muir KR, Doherty M, Jones AC, O'Reilly SC, et al. (2002) Home based exercise programme for knee pain and knee osteoarthritis: randomised controlled trial. BMJ 325(7367): 752.v
- Simkin PA, Huang A, Benedict RS (1990) Effects of exercise on blood flow to canine articular tissues. J Orthop Res 8(2): 297-303.
- Gerber LH (1990) Exercise and arthritis. Bull Rheum Dis 39(6): 1-9.
- James MJ, Cleland LG, Gaffney RD, Proudman SM, Chatterton BE (1994) Effect of exercise on 99mTc-DTPA clearance from knees with effusions. J Rheumatol 21(3): 501-504.
- Hawley DJ (1995) Psycho-educational interventions in the treatment of arthritis.Baillieres Clin Rheumatol 9(4): 803-823.
- Brooks M, Beaulieu J, Heiderscheit B, Severson HH, Wille CM, et al. (2014) Web-based therapeutic exercise resource center as a treatment for knee osteoarthritis: a prospective cohort pilot study. BMC Musculoskeletal Dis 15: 158.
- Barwick PA, Swezey RL (1982) Physical therapies in arthritis. Which to choose, when to use, how not to abuse. Postgrad Med 72(3): 223-233.
- Petrella RJ. (1999) Exercises for patients with knee osteoarthritis. Phys Sportsmed 27: 109-111.
- Kovar PA, Allegrante JP, MacKenzie CR, et al. (1992) Supervised fitness walking in patients with osteoarthritis of the knee. A randomized, controlled trial. Ann Int Med 16: 529-534.
- Peloquin L, Bravo G, Gauthier P, et al. (1999) Effects of a cross-training exercise program in persons with osteoarthritis of the knee a randomized controlled trial. J Clin Rheumatol 5: 126-136.
- Marks R. (2012) Knee osteoarthritis and exercise adherence: a review. Curr Aging Sci 5: 72-83.
- Skou ST, Rasmussen S, Laursen MB, Rathleff MS, Arendt-Nielsen, et al. (2015) The efficacy of 12 weeks non-surgical treatment for patients not eligible for total knee replacement: a randomized controlled trial with 1-year follow-up. Osteoarthritis Cartilage 23:1465-1475.
- Wade J, Liang MH. (1988) Management of non-inflammatory musculoskeletal disorders in the elderly. Complementary Ther 14: 38-43.
- Tanaka R, Ozawa J, Kito N, Moriyama H. (2013) Efficacy of strengthening or aerobic exercise on pain relief in people with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil 27: 1059-1071.
- Wu SF, Kao MJ, Wu MP, Tsai MW, Chang WW. (2011) Effects of an osteoarthritis self-management programme. J Adv Nurs 67:1491-1501.
- Basedow M, Williams H, Shanahan EM, Runciman WB, Esterman A (2015) Australian GP management of osteoarthritis following the release of the RACGP guideline for the non-surgical management of hip and knee osteoarthritis. BMC Res Notes 8: 536.
- Andriacchi TP, Favre J. (2014) The nature of in vivo mechanical signals that influence cartilage health and progression to knee osteoarthritis. Curr Rheumatol Rep 16: 463.
- Robbins SM, Birmingham TB, Callaghan JP, Jones GR, Chesworth BM, et al . (2011) Association of pain with frequency and magnitude of knee loading in knee osteoarthritis. Arthritis Care Res 63(7): 991-997.
- Van Manen MD, Nace J, Mont MA. (2012) Management of primary knee osteoarthritis and indications for total knee arthroplasty for general practitioners. J Am Osteopath Assoc 112: 709-715.
- Waller B, Ogonowska-Slodownik A, Vitor M, Lambeck J, Daly D, et al. (2014) Effect of therapeutic aquatic exercise on symptoms and function associated with lower limb osteoarthritis: systematic review with meta-analysis. Phys Ther 94(10): 1383-1395.
- Power JD, Badley EM, French MR, Wall AJ, Hawker GA. (2008) Fatigue in osteoarthritis: a qualitative study. BMC Musculoskelet Disord 9: 63.
- Williamson EM, Marshall PH. (2014) Effect of osteoarthritis on accuracy of continuous tracking leg movement. Percept Mot Skills 118: 162-182.
- Athanasiou KA, Responte DJ, Brown WE, Hu JC. (2015) Harnessing biomechanics to develop cartilage regeneration strategies. J Biomech Eng Feb 1;137(2):020901.
- Felson DT. (2013) Osteoarthritis as a disease of mechanics. Osteoarthritis Cart 21: 10-15.
- Loeser RF Jr. (2000) Aging and the etiopathogenesis and treatment of osteoarthritis. Rheum Dis Clin North Am 26(3): 547-567.
- Brandt K D (1998) The importance of non pharmacologic approaches in management of osteoarthritis. Am J Med 105(1): 39S-44S.
- Roos EM, Arden NK. (2015) Strategies for the prevention of knee osteoarthritis. Nat Rev Rheumatol Oct 6. doi: 10.1038/nrrheum.2015.135.
- Huang KH, Hsieh RL, Lee WC (2015) Pain, physical function, and health in patients with knee osteoarthritis. Rehabil Nurs doi: 10.1002/rnj.234.
- Anwer S, Alghadir A, Brismée JM (2015) Effect of home exercise program in patients with knee osteoarthritis: a systematic review and meta-analysis. J Geriatr Phys Ther 38(1): 1-11.
- Harris H, Crawford A. (2015) Recognizing and managing osteoarthritis. Nursing. 45 (1):36–42.
- Smink AJ, Bierma-Zeinstra SM, Schers HJ, et al. (2014) Non-surgical care in patients with hip or knee osteoarthritis is modestly consistent with a stepped care strategy after its implementation. Int J Qual Health Care 26:490-498.
- Dias RC, Dias JM, Ramos LR. (2003) Impact of an exercise and walking protocol on quality of life for elderly people with OA of the knee. Physiother Res Int 8: 121-130.
- Shamliyan TA, Wang SY, Olson-Kellogg B, Kane RL. (2012) Physical therapy interventions for knee pain secondary to osteoarthritis [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2012 Nov.Available from http://www.ncbi.nlm.nih.gov/books/NBK114568/
- Walker J. (2011) Management of osteoarthritis. Nurs Older People 23: 14- 19.
- Alami S, Boutron I, Desjeux D, Hirschhorn M, Meric G, et al. (2011) Patients' and practitioners' views of knee osteoarthritis and its management: a qualitative interview study. PLoS One 6(5):e19634. doi:10.1371/journal.pone.0019634
- Benhamou M, Baron G, Dalichampt M, Boutron I, Alami S, et al. (2013) Development and validation of a questionnaire assessing fears and beliefs of patients with knee osteoarthritis: the Knee Osteoarthritis Fears and Beliefs Questionnaire (KOFBeQ). PLoS One 8(1): e53886. doi: 10.1371/journal. pone.0053886.
- Benhamou M, Boutron I, Dalichampt M, Baron G, Alami S, et al. (2013) Elaboration and validation of a questionnaire assessing patient expectations about management of knee osteoarthritis by their physicians: the Knee Osteoarthritis Expectations Questionnaire. Ann Rheum Dis 72: 552-559. doi: 10.1136/annrheumdis-2011-201206.
- Barr A, Conaghan PG. (2012) Osteoarthritis: a holistic approach. Clin Med 12: 153-155.





