Study of Prevalence of Martin-Gruber Anomaly in Patients with Carpal Tunnel Syndrome
Ayramlou H1, Najmi S2*, Yazdchi M1, Naeimi M3, Pourabolghasem S2
1 Professor of Neurology; Department of Neurology, Tabriz University of Medical Science, Iran.
2 Assistant Professor of Neurology, Department of Neurology, Tabriz University Of Medical Science, Iran.
3 Assistant Professor of Neurology, Department of Neurology, Gholestan University of Medical Science, Iran.
*Corresponding Author
Safa Najmi,
Assistant Professor of Neurology,
Department of Neurology,
Tabriz University of Medical Science, Iran.
E-mail: safanajmi@yahoo.com
Article Type : Research Article
Received: September 15, 2015; Accepted: November 16, 2015; Published: November 18, 2015
Citation: Najmi S, et al., (2015) Study of Prevalence of Martin-Gruber Anomaly in Patients with Carpal Tunnel Syndrome. Int J Chronic Dis Ther 1(2) 5-8.doi: dx.doi.org/10.19070/2572-7613-150002
Copyright: Najmi S© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Median-Ulnar connection in the forearm, also known as the Martin-Gruber communication (MGC), is a common anatomic nerve anomaly with the incidence from 5% to 34% in the normal population.
Knowledge of this anomaly is of crucial importance in evaluation of injuries of Median and Ulnar nerves; as well as in accurate interpretation of the nerve conduction velocity of these nerves.
This study aimed at evaluating the frequency of martin - Gruber communication and its common types in patients with Carpal Tunnel Syndrome (CTS).
151 patients with definite diagnosed Carpal Tunnel Syndrome by electro-diagnostic method (123 females and 28 males with the mean age of 46.42+/_11.21 years) were enrolled in the study over a 13 months period. 19 patients (12.6 %) -13 females, 6 males-had MGC. In 285 upper extremities with carpal tunnel syndrome, 25 (8.8%) cases had martin - Gruber communication. Types 1, 2 and 3 of this anomaly were seen in 7 (43.8%), 14 (87.5%), 6 (37.5%) patients respectively.
In our study the prevalence of Martin - Gruber connection in the patients with carpal tunnel syndrome was within the same range as in literature, however lower than the mean reported value. MGC Type 2 was the most common type in patients with CTS.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Carpal Tunnel Syndrome; Martin-Gruber Anomaly; Nerve Conduction Velocity.
Introduction
Median-Ulnar connection is the most common peripheral nerve anomaly, with autosomal dominant inheritance, known as Martin- Gruber connection (MGC). Actually, this anomaly is crossover of mainly motor fibers of median nerve to Ulnar in forearm [1, 6, 7], which may produce changes in the innervations of the upper limb muscles, mainly motor part of intrinsic muscles in the hand [2]. Some types of MGC have been recognized. Anastomosis in which the branch anastomotic originates proximally in the median nerve and unites distally in the ulnar nerve is known as Median- Ulnar anastomosis. It can arise between the branches destined to the deep flexor muscle of the fingers, or directly in the median to the ulnar nerve, or between the Anterior Inter-osseous and ulnar nerves or in combinations between these types of anastomoses. However, another type of anastomosis can happen in the forearm. When the anastomotic branch originates proximally in ulnar nerve and unites distally to median nerve is simply called anastomosis of Ulnar-Median type, or Martin-Gruber reverse anastomosis or Marinacci anastomosis.
MGC in almost 10-40% is bilateral, but in the unilateral form, it is commonly seen in right [4, 9].
There is no significant difference between males and females with respect to gender distribution [4, 9].
Also there are very studies about prevalence of Martin-Gruber anomaly, but there are a few studies about prevalence of this anomaly in patients with carpal tunnel syndrome such as Lyer and et al study [13] and Simonetti and et al study [14]. With respect to these studies prevalence of Martin-Gruber anomaly in patients with carpal tunnel syndrome is 1/54% to 26% [10].
In conditions affecting the nerves that supply intrinsic muscles of the hand, this anastomosis can cause confusion in the diagnosis since the crosses of axons can innervate the intrinsic muscles supplied by the ulnar nerve, median nerve or both (KAZAKOS, SMYMIS, XARCHAS et al., 2005). A typical example is Carpal Tunnel Syndrome which symptoms may be incomplete or exacerbate due the existence of these anastomoses, because a modification happens in the upper limb innervation. Moreover, a traumatic injury in forearm nerves might amiss be interpreted as a partial injury of the medium nerve or ulnar nerve (BOLUKBASI, TURGUT and AKYOL, 1999).
Due to high prevalence of Carpal Tunnel syndrome and partially high prevalence of Martin-Gruber anomaly, co morbidity of them can alter the results of evaluations like electro diagnostic tests and plan of treatment of CTS. So, orientation and recognition of MGC may be helpful in treatment of median and ulnar nerves lesions [9].
Purposes of this study are:
- Prevalence of Martin-Gruber connection in patients with carpal tunnel syndrome
- Prevalence determination of types of Martin-Gruber connection
- Determination of gender distribution of martin-Gruber connection in patients with carpal tunnel syndrome.
Materials and Methods
We evaluated presences of Martin-Gruber connection in patients with Carpal Tunnel Syndrome through a prospective analytic-descriptive study, during 13 months study in Neuro-diagnostic ward of Tabriz Imam Reza hospital, Iran. Clinically and para-clinically diagnosed patients with Carpal Tunnel Syndrome were studied for Martin-Gruber connection by electro-diagnostic tests. Then the data were analyzed with respect to age, sex and side of anomaly in patients. All the patients with any disease or condition that may impact on Carpal Tunnel Syndrome, like Hypothyroidism, Uremia, Diabetes, Trauma, any history of Neuropathies, Hypercholesterolemia, Vasculopathies, etc. were excluded from project.
We evaluated all the patients by MEDELEK EMG 4 cannel procedure and measured all the Sensory and Motor Nerve action potentials, Velocities, latencies and late responses of Median and Ulnar Nerves bilaterally with Needle electromyography of muscles in territory of those nerves.
Results
151 patients with documented CTS via EMG_NC were evaluated for Martin-Gruber Connection. We found the electro-neuro-diagnostic evidence of MGC in 19 persons (12.5%) from the all-151 patients with CTS.
From the totally 302 evaluated upper limbs in 151 patients, 285 upper limbs had CTS and from the involved limbs, 25 forearms (8.77%) had MGC.
Mean age in our patients with Martin-Gruber connection was 45.06 +/- 8.43 and in rest of patients in our group was 46.65+/- 11.64;
We found MGC in 14 right forearm and 11 left side. From the all-19 persons with MGC, 4 patients had bilaterally MGC and the rest of them were unilateral. From whom with MGC, 13 persons were female and 6 were male (female: male was more than 2) and the same gender ratio was true about patients CTS in our study group (68.4% females, 31.6% male);
In patients with martin-Gruber connection, 43.8% had Type 1; 87.5% had Type 2 and 37.5% had Type 3 of MGC. It means that some patients (limbs) have had more than one type of MGC.

Table
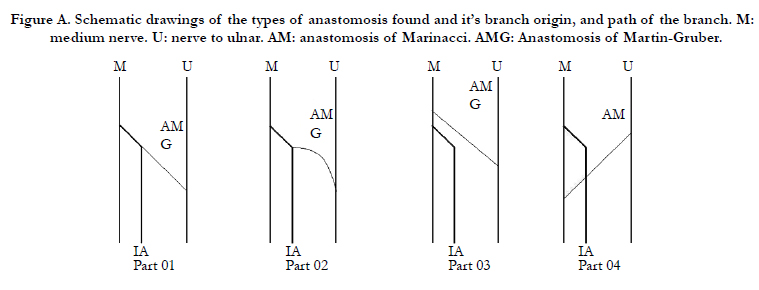
Figure A. Schematic drawings of the types of anastomosis found and it’s branch origin, and path of the branch. M: medium nerve. U: nerve to ulnar. AM: anastomosis of Marinacci. AMG: Anastomosis of Martin-Gruber.
Discussion
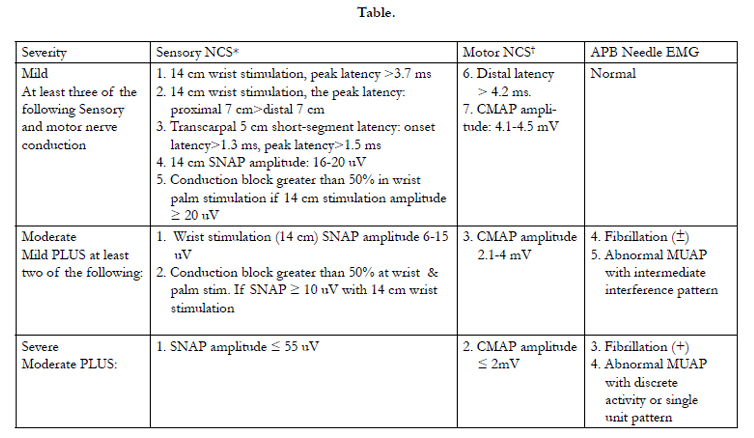
Carpal tunnel syndrome (CTS) arises from the intermittent or continuous compression or entrapment of the median nerve as it passes through the carpal tunnel from the wrist to the hand. Increased pressure on the median nerve in the carpal tunnel can result in progressive sensory and motor disturbances in parts of the hand innervated by this nerve, leading to pain and loss of function. (Sluiter 2001). Symptoms of CTS include numbness (anesthesia) and tingling (paresthesia) in the anatomic distribution of the median nerve (the area including the thumb, index finger, long finger, and radial half of the ring finger) (Stevens 1999). A nocturnal symptom of sensory disturbance is considered a classic manifestation of carpal tunnel syndrome. Patients frequently complain of pain in the wrist or hand at night or after frequent use of the hands or fingers, commonly relieved by "shaking it out" (Hennessey 1997). Electro-diagnostic studies (EDS) are also used in the diagnosis of carpal tunnel syndrome. Electro-diagnostic studies include electromyography (EMG) and the nerve conduction study (NCS). Due to Electro-diagnostic methods, CTS generally is classified to 3 stages that are summarized in Table below [28].
In the forearm, median and ulnar communication was first described by the Swedish anatomist Martin (in 1763) and later by Gruber (in 1870) and thus referred to as the Martin-Gruber Anastomosis (MGA) [31]. This anastomosis involves axons leaving either the main trunk of median nerve or the anterior inter-osseous nerve, crossing through the forearm to join the main trunk of the ulnar nerve and ultimately innervating the intrinsic hand muscles [31].
In the literature, there are several studies on MGA classification; by different techniques [anatomical [5, 21], histological [20] and electrophysiological [19].
Anatomically there are three types MGC. In Type 1 anastomosis the crossover fibers terminate in the Hypothenar muscles, in the Type 2, in the FDI, and in the Type 3, in the Thenar muscle group. [17]. Due to literature, Type 2 is the most common type [17].
Its reported incidence differs between physiologic and anatomic studies. In the former it has been described as occurring in 5-40% of cases [6, 18, 19] whereas anatomic studies report a narrower range of 10-30.6% [33]. The MGA suggested that unilateral MGA occurs more often in the right side than the left [20]. But no differences were reported with respect to the frequencies of MGA or MGA types for the sexes [17].
In the literature, some researchers cited the clinical importance of MGA [19, 20-23]. The intrinsic muscles of the hand were completely unaffected by median lesions. A lesion of the median nerve situated proximal to the departure of the communicating branch would affect the median Thenar muscles, whereas a lesion below that level would not [3]. Brandsma et al. [23] reported that the clinical importance of this anastomosis is that an isolated ulnar nerve lesion at the elbow may produce an unusual pattern of intrinsic muscle paralysis. The MGA has clinical significance for understanding median nerve lesion and the carpal tunnel syndrome. In addition, Niedenfuhr et al. [24] cited that the intramuscular MGA because the intramuscular course of a nerve is a potential compression site, the cases presented in this study may have an additional clinic implication.
Conclusion
MGC may be source of confusion in diagnosis and management of much neuropathic process in upper limbs like CTS. Normal motor latencies are obtained in such cases. However, there are certain clues to the correct diagnosis: - Median nerve stimulation at the elbow evokes a thenar CMAP with an initial positive deflectin; -A Thenar CMAP with two peaks in the negative phase on stimulation at the elbow; and - An erroneously normal proximal motor latency in the Median nerve with prolongation of distal motor latency results in a spuriously fast conduction velocity by calculation.
Due to partially high incidence of this anastomosis and its role in confusing in some diagnosis of some pathologic process, MGC must be keeping in mind in management of carpal tunnel syndrome to correct diagnosis and select suitable treatment.
References
- Ashworth NL, Sucher BM, Talavera F, Foye PM (2004) E-medicine 8(21): 1-11.
- Felippe MM, Telles FL, Soares ACL, Felippe FM (2012) Anastomosis between median nerve and ulnar nerve in the forearm. J Morphol Sci 29(1):23-26.
- De-Krom MC, Knipschild PG, Kester AD, Thijs CT, Boekkooi PF, et al. (1992) Carpal tunnel syndrome: prevalence in the general population. J Clin Epidemiol 45(4): 373-376.
- Simon R, Aminoff M, Greenberg D (1999) Clinical Neurology. (4th edtn), Lange, Stanford, 170-173.
- Srinivasan R, Rhodes J (1981) The median-ulnar anastomosis (Martin- Gruber) in normal and congenitally abnormal fetuses. Arch Neurol 38(7): 418-419.
- Martin F (1763) Tal Om nervers allmanna agenskaler i manniskans kropped Stockholm: L. Salvius 1: 253.
- Gruber W (1870) Über die verbindung des nervus medianus mit dem nervus ulnaris an unterarme des menschen und der saugethiere. Arch Anat Physiol 37: 501-522.
- Shapiro BE (1998) Electromyograph and neuromuscular disorders. Butterworth- Heinemann, Germany. 77-81.
- Erdem HR, Ergun S, Erturk C, Ozel S (2002) Electrophysiological evaluation of the incidence of Martin-Gruber anastomosis in healthy subjects. Yonsei Med J 43(3): 291-295.
- Oh SJ (2003) Electrophysiology. (3rd edtn), Lippincott Williams & Wilkins, USA. 345-352.
- Wilma K (1997) Anomalous hand innervation in carpal tunnel syndrome. Electroencephal Clin Neurophysiol 103(1): 209.
- Meenakshi-Sundaram S, Sundar B, Arunkumar MJ (2003) Marinacci communication: an electrophysiological study. Clin Neurophysiol 114(12): 2334-2337.
- Iyer V, Fenichel GM (1976) Normal median nerve proximal latency in carpal tunnel syndrome: a clue to coexisting Martin-Gruber anastomosis. J Neurol Neurosurg Psychiatry 39(5): 449-452.
- Simonetti S (2001) Electrophysiological study of forearm sensory fiber crossover in Martin-Gruber anastomosis. Muscle Nerve 24(3): 380-386.
- Sun SF, Streib EW (1983) Martin-Gruber anastomosis: electromyographic studies. Part II. Electromyogr Clin Neurophysiol 23(4): 271-285.
- Uchida Y, Sugioka Y (1992) Electrodiagnosis of Martin-Gruber connection and its clinical importance in peripheral nerve surgery. J Hand Surg (Am)17(1): 54-59.
- Erdem HR, Ergun S, Erturk C, Ozel S (2002) Electrophysiological evaluation of the incidence of Martin-Gruber anastomosis in healthy subjects. Yonsei Med J 43(3): 291-295.
- Piza-Katzer H (1976) Familial occurence of Martin-Gruber anastomosis. Handchirurgie 8(4): 215-218.
- Lee KS, Oh CS, Chung IH, Sunwoo IN (2005) An anatomic study of the Martin-Gruber anastomosis: electrodiagnostic implications. Muscle Nerve 31(1): 95-97.
- Shu HS, Chantelot C, Oberlin C, Alnot JY, Shao H (1999) Martin-Gruber communicating branch: anatomical and histological study. Surg Radiol Anat 21(2): 115-118.
- Rodriguez-Niedenfuhr M, Vazquez T, Parkin I, Logan B, Sanudo JR (2002) Martin-Gruber anastomosis revisited. Clin Anat 15(2): 129-134.
- Marur T, Akkin SM, Alp M, Demirci S, Yalcin L, et al. (2005) The muscular branching patterns of the ulnar nerve to the flexor carpi ulnaris and flexor digitorum profundus muscles. Surg Radiol Anat 27(4): 322-326.
- Brandsma JW, Birke JA, Sims DS Jr (1986) The Martin-Gruber innervated hand. J Hand Surg Am 11(4): 536-539.
- Rodriguez -Niedenfuhr M, Vazquez T, Ferreira B, Parkin I, Nearn L, et al. (2002) Intramuscular Martin- Gruber anastomosis. Clin Anat 15(2): 135-138.
- Budak F, Gonenc Z (1999) Innervation anomalies in upper and lower extremities (an electrophysiological study). Electromyogr Clin Neurophysiol39(4): 231-234.
- Taams KO (1997) Martin-Gruber connections in South Africa. An anatomical study. J Hand Surg Br 22(3): 328-330.
- Nakashima T (1993) An anatomic study on the Martin-Gruber anastomosis. Surg Radiol Anat 15(3): 193-195.
- Stevens JC (1997) AAEM minimonograph #26: the electrodiagnosis of carpal tunnel syndrome. American Association of Electrodiagnostic Medicine.Muscle Nerve 20(12): 1477-1486.
- Ashworth NL (2004) Carpal tunnel syndrome: Clinical evidence. BMJ 16(11): 1417-1434.
- Aurora SK, Ahmad BK, Aurora TK (1998) Silent period abnormalities in carpal tunnel syndrome. Muscle Nerve 21(9): 1213-1215.
- Nadire UNVER DOGAN Ismihan Ilknur UYSAL Muzaffer SEKER Published online 14 March, 2009 © http://www.neuroanatomy.org the communications between the ulnar and median nerves in upper limb
- Kayamori R (1987) Electrodiagnosis in Martin-Gruber anastomosis. Nihon Seikeigeka Gakkai Zasshi 61(12): 1367-1372.
- Sarikcioglu L, Sindel M, Ozkaynak S, Aydin H (2003) Median and ulnar nerve communication in the forearm: an anatomical and electrophysiological study. Med Sci Monit 9(9): BR351-BR356.
- Amoiridis G, Vlachonikolis IG (2003) Verification of the median-to-ulnar and ulnar-to-median nerve motor fiber anastomosis in the forearm: an electrophysiological study. Clin Neurophysiol 114(1): 94-98.
- Shu H, Chantelot C, Oberlin C, Alnot JY, Shao H (1999) Anatomic study and review of the literature on the Martin Gruber anastomosis. Morphologie 83(260): 71-74.





